Treatment of women with diastasis recti
HTA Report
 Share on Facebook
Share on Facebook
 Share on LinkedIn
Share on LinkedIn
 Share via Email
Share via Email
Conclusions
- The available evidence is insufficient to evaluate the effect of physiotherapeutic or surgical interventions for treating women with symptomatic diastasis recti.
- There is insufficient evidence to determine the cost-effectiveness of treatments for diastasis recti in women.
- There is a need for more research with a prospective and controlled study design to guide clinicians on if and how diastasis recti should be treated, and which women will benefit from physiotherapy or surgery. Future clinical trials should further evaluate outcomes such as physical function, disability, and health related quality of life.
Background
Diastasis of the rectus abdominis muscle (DRAM) occurs when the midline fascia (linea alba) widens. It is a common condition in women after pregnancy but can also occur after significant weight loss or due to other causes. In some women the gap between the abdominal muscles spontaneously close during the first year after childbirth. The proportion of women with a persisting DRAM is not known, nor are the long-term consequences of the condition understood. The symptoms caused by DRAM are currently uncertain, but some studies indicate it may be associated with abdominal pain, impaired physical function, and reduced health related quality of life. DRAM can also affect the aesthetic appearance negatively and has been suggested to be linked to pain in the lower back and pelvis as well as urogenital conditions.
Treatment usually starts with physical exercise to reduce the slack of linea alba and improve the ability of the abdominal and core muscles to maintain stability of the torso. In some cases, where physical treatment fails, surgical correction can be considered. There is currently no clear consensus in Sweden regarding how or when DRAM should be treated, correspondingly there are regional differences in the care provided.
Aim
This systematic review was conducted to assess the current evidence for treatment of symptomatic DRAM in women, this includes:
- the effect of interventions for treating DRAM: reduction of the inter-recti distance (IRD), alleviation of symptoms, improvement of function and health related quality of life
- the adverse effects of treatments for DRAM
- the cost-effectiveness of treatments for DRAM
The report also includes a chapter on ethical considerations.
Method
A systematic review conducted in accordance with the PRISMA statement. The protocol is registered in Prospero (CRD42021236961). The certainty of evidence was assessed with GRADE.
The chapter on ethical considerations is based on discussions with the clinical experts involved in the project as well as with a focus group. The focus group consisted of women who had experienced DRAM personally or who were a close relative to a woman who had experienced DRAM. The purpose was to bring up important ethical aspects to consider in relation to DRAM and possible treatment of the condition and its consequences.
Inclusion criteria
Population:
Women with symptomatic DRAM after pregnancy, weight loss or caused by unspecified/unknown causes.
All participants must have a clinical diagnosis of DRAM of >2 cm or two finger widths. Women must comprise at least ¾ of the study population, if not reported separately.
Intervention:
Methods intended to treat DRAM or consequences of the condition: relevant modalities include physiotherapy and surgery. The methods must be deemed to be relevant for the Swedish health-care system.
Control:
No treatment, sham treatment, treatment as usual or an active treatment option.
Outcome:
- Diastasis (curative effect, diastasis width, recurrence)
- Effect on symptoms
- Physical function
- Disability
- Health related quality of life
- Adverse effects and complications, as reported in the included intervention studies
Study design: Prospective clinical trials, with or without randomisation, and with a control group.
Language: Danish, English, Norwegian, Swedish.
Search period: From 1990 to 2021. Final search August 2021.
Databases searched: Medline, EMBASE, Cochrane Library (CDSR, DARE & CENTRAL), PEDRO and Cinahl
Client/patient involvement: Yes
Results
Outcomes from five RCT:s (including one quasi-RCT) are included in this systematic review (Figure 1). Four focused on physiotherapeutic interventions and one on a comparison of two surgical interventions.
| BAS = Body Appreciation Scale; CI = confidence interval; HRQoL = Health-related quality of life; MD = mean difference; n.s. = non-significant result; PFDI-20 = Pelvic Floor Distress Inventory, 20-items; RCT = Randomised Controlled Trial; RDQ = Roland-Morris Disability Questionnaire; reps. = repetitions; RR = relative risk; SD = standard deviation; SF-36 = Medical Outcomes Study 36-item Short-Form Health Survey; VHPQ = Ventral Hernia Pain Questionnaire. A RR over 1 indicates a higher proportion of resolution in DRAM in the intervention group compared to the control group. B BAS. A positive value indicates a better outcome for the combination treatment. Range 1–5, higher score indicates greater body appreciation. C A positive value indicate a better outcome for the combination treatment compared to physical exercise alone. D Results from 1 RCT with 36 participants. E A positive value indicates a worse outcome for the intervention, range 0 (least distress) to 300 (greatest distress). F A negative value indicates a better outcome for the intervention group compared to the control group, range 0 (no disability) to 24 (severe disability). G RR over 1 indicate a higher proportion of recurrence in the mesh group compared to the suture groups. 1 Risk of Bias –2. Few studies with relatively few participants. Concerns about the RoB for one study. One study with per protocol analysis. 2 Directness –1. Both studies are from a specific context and have included a narrowly defined population. 3 Only one study with relatively few participants, insufficient evidence to support any conclusions. |
|||
| Outcome | Number of studies and participants | Results MD/RR (95% CI) | Certainty of evidence |
|---|---|---|---|
| Physical exercise compared with no treatment, end of treatment | |||
| Width of DRAM | 1 RCT n=17 |
MD (SD): –1.09 cm (0.63) vs. –0.13 cm (0.31) (p≤0.05) |
Very low3 ⊕◯◯◯ |
| Resolution of DRAM (<2 fingerwidths) | 1 RCT n=96 |
RR: 1.11 (0.5 to 2.49) A (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Physical function – Pelvic floor (PFDI-20) | 1 RCT n=13 |
MD: 2.80 (–10.01 to 15.61)E (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Disability – Pain related disability (RDQ) | 1 RCT n=13 |
MD: –0.30 (–5.63 to 5.03)F (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Physical exercise in combination with taping compared with no treatment, end of treatment | |||
| Reduction in width of DRAM | 1 RCT n=12 |
MD (SD): –1.07 cm (0.66) vs. –0.13 cm (0.31) (p≤0.05) |
Very low3 ⊕◯◯◯ |
| Physical function – Pelvic floor (PFDI-20) | 1 RCT n=10 |
MD: 14.80 (–11.65 to 41.25)E (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Disability – Pain related disability (RDQ) | 1 RCT n=10 |
MD: –1.00 (–6.26 to 4.26)F (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Taping compared with no treatment, end of treatment | |||
| Width of DRAM | 1 RCT n=15 |
MD (SD): –0.29 cm (0.28) vs. –0.13 cm (0.31) (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Physical function – Pelvic floor (PFDI-20) | 1 RCT n=9 |
MD: 10.40 (–3.67 to 24.47)E (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Disability – Pain related disability (RDQ) | 1 RCT n=9 |
MD: –0.30 (–6.99 to 6.39)F (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Physical exercise in combination with NMES compared with physical exercise, end of treatment | |||
| Width of DRAM | 1 RCT & 1 quasi-RCT n=93 |
MD: –0.36 cm (–0.46 to –0.26) |
Very low1,2 ⊕◯◯◯ |
| Symptoms – body image (BAS) | 1 RCT n=36 |
MD: 0.71 (0.52 to 0.90)B (p≤0.05) |
Very low3 ⊕◯◯◯ |
| Physical function – abdominal muscle strength (dynamometer) | 1 RCT & 1 quasi-RCT n=93 |
Peak torque (Nm): MD: 5.14 (3.29 to 6.99)C Average power (W): MD: 3.85 (2.64 to 5.07)C Total work (J): MD: 6.05 v(4.14 to 7.95)C Endurance (reps.)D: MD: 8.33 (6.38 to 10.28)C |
Very low1,2 ⊕◯◯◯ |
| Physical exercise compared with surgical treatment with mesh implant, 3 months after treatment | |||
| Physical function – effect of pain on function (VHPQ) | 1 RCT n=57 |
No significant difference between the groups for 8/9 items on the VHPQ | Very low3 ⊕◯◯◯ |
| Physical exercise compared with surgical treatment with suture alone, 3 months after treatment | |||
| Physical function – disability (VHPQ) | 1 RCT n=58 |
No significant difference between the groups for any of the items on the VHPQ | Very low3 ⊕◯◯◯ |
| Surgical treatment with mesh implant compared with suture alone, 1 year after treatment | |||
| Recurrence of DRAM (≥3 cm) | 1 RCT n=57 |
RR: 3.10 (0.13 to 73.12), (n.s., p>0.05)G |
Very low3 ⊕◯◯◯ |
| Physical function – abdominal muscle strength (dynamometer) | 1 RCT n=56 |
Difference between groups reported to be n.s. (p>0.05) | Very low3 ⊕◯◯◯ |
| Physical function – abdominal muscle strength (self-reported) | 1 RCT n=56 |
Median (SD): 7 (2.62) vs. 8 (2.08) (n.s., p>0.05) |
Very low3 ⊕◯◯◯ |
| Physical function – effect of pain on function (VHPQ) | 1 RCT n=56 |
No statistically significant difference between the groups for 6/9 items on the VHPQ | Very low3 ⊕◯◯◯ |
| HRQoL (SF-36, reported for 8 subscales) | 1 RCT n=57 |
3/8 subscales (GH, VT & MH) indicate benefit for mesh implant (p≤0.05). | Very low3 ⊕◯◯◯ |
Health Economic Assessment
No studies on the cost-effectiveness of interventions were identified. The cost-effectiveness of treatments could not be estimated due to the lack of evidence on treatment effects. Studies on the effect of treatment as well as the direct and indirect costs associated with treatment of DRAM are needed to estimate the cost-effectiveness of physiotherapeutic and surgical treatment of DRAM.
Ethics
In brief, it is important that women with symptomatic DRAM receives a good level of care and that the symptoms attributed to DRAM are examined. There is a risk that the lack of evidence for the treatment of DRAM may lead to women not receiving adequate care, or qualitative differences in the care provided. For healthcare providers the current situation is challenging due to the lack of evidence for treatments, and the insufficient knowledge regarding the symptoms caused by DRAM or of the long-term consequences of DRAM if left untreated. The condition has potentially both aesthetic and medical consequences, further complicating the clinical assessment.
Discussion
Only five studies were identified that reported the effects of treatment of DRAM in women. The studies were heterogenous with respect to the treatment, the control, and the outcomes reported. Due to this heterogeneity only the results from two studies could be combined. The certainty of the evidence is therefore very low (⊕◯◯◯) across all interventions and outcomes.
Different forms of physiotherapy were investigated in four studies. In general, the women had a moderate DRAM and the treatment started within a few months post-partum. However, the symptoms attributed to the condition at enrollment were not reported. This leads to uncertainty on the effect of treatment for women with more severe or more persistent DRAM, or for those reporting specific symptoms. None of the studies reported adverse events of the treatment, and only one study reported a long term follow up after the end of the treatment.
One study compared surgical correction of DRAM with reinforcement of the linea alba using a surgical mesh implant to using sutures alone, in parous women. The study also reported the effect of the two surgical techniques to that of physical exercise on physical function (VHPQ), at the end of the 3-month exercise programme. For the patients undergoing surgery, adverse effects were reported at 3 months after surgery and the outcomes were reported for up to one to five years after the intervention. However, the lack of more studies limits the certainty of the evidence.
Further research is needed to assess the effect of interventions for DRAM, and on patient groups with different indications for treatment. There is a need for studies which assess how the treatment effect is affected by factors such as age, cause of and duration of the DRAM. Clinical studies need to put greater emphasis on evaluating the effect of treatment on potential consequences of DRAM by including outcomes on physical function, disability, and health-related quality of life. Also, studies investigating the long-term effects and cost-effectiveness of treatments are needed.
The lack of evidence should not be interpreted as a lack of effect for the treatments, at present the evidence is too limited to draw any conclusion. For a study to be included in this review, the participants had to have a DRAM of more than 2 cm. However, a DRAM of more than 2 cm may not cause any symptoms and should not in itself be regarded as a condition that requires medical treatment.
Conflicts of Interest
In accordance with SBU’s requirements, the experts and scientific reviewers participating in this project have submitted conflicts of interest statements. These documents are available at SBU’s secretariat. SBU has determined that the conditions described in the submissions are compatible with SBU’s requirements for objectivity and impartiality.
The full report in Swedish
The full report in Swedish Behandling av rektusdiastas hos kvinnor
Project group
Experts
- Karin Strigård, MD, Professor, Department of Surgical and Perioperative Sciences, Umeå University
- Catharina Gustavsson, Physiotherapist, Associate professor, Center for clinical research Dalarna, Uppsala University
- Trude Staalesen, MD, PhD, Volvat medisinske senter Oslo, Norway
- Ulrik Kihlbom, Associate professor, Centre for Research Ethics & Bioethics, Uppsala University.
SBU
- Martin Norman, Project Manager
- Charlotta Ryk, Assistant Project Manager
- Thérèse Eriksson, Health Economist
- Sara Fundell, Project Administrator
- Ann Kristine Jonsson, Information Specialist
Flow chart
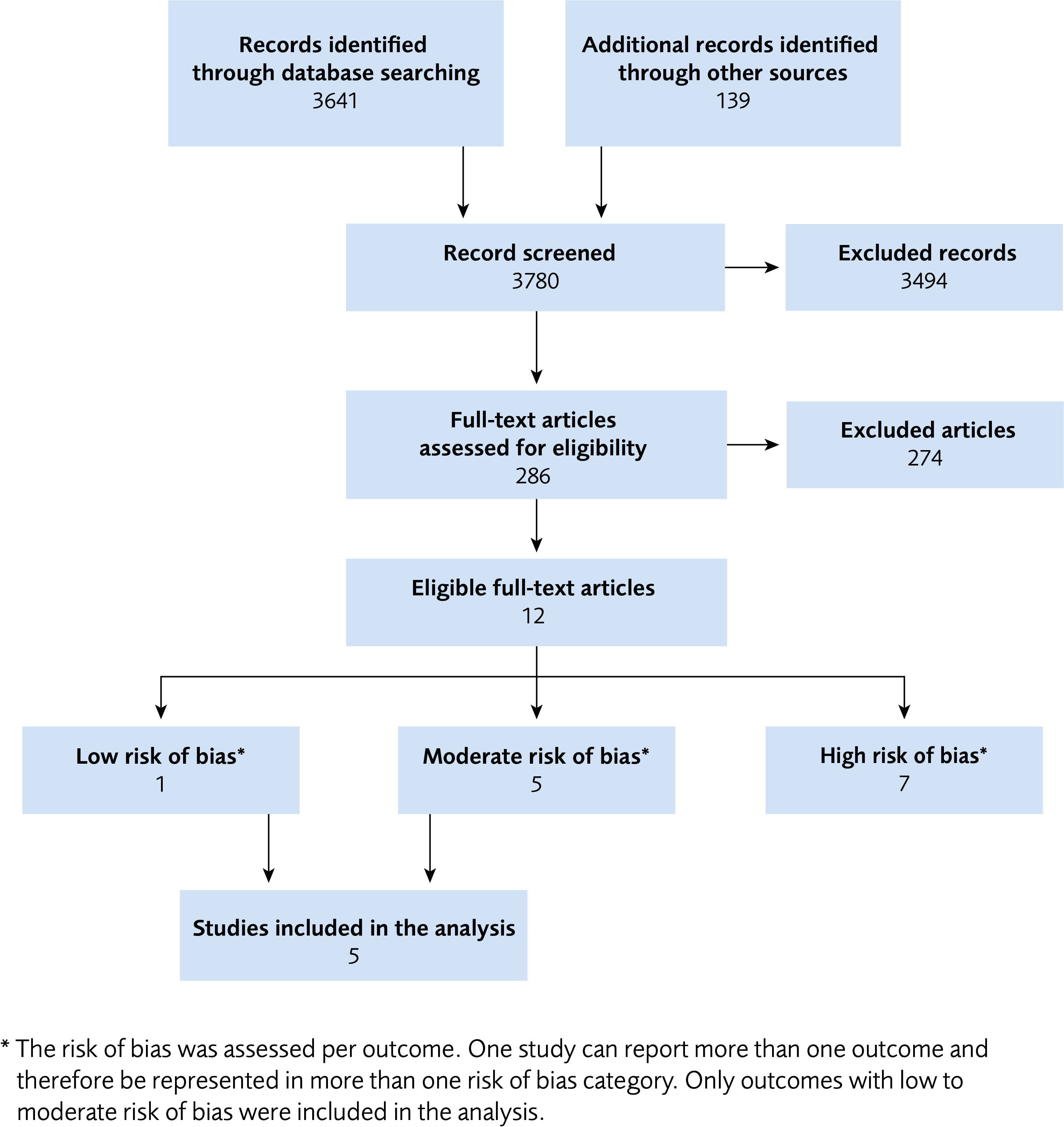
Figure 1 Flow chart for the literature review process.
Appendices
- Search strategies (pdf)
- Excluded articles (pdf)
- Risk of bias assessments (pdf)
- Characteristics of included studies (pdf)
References
- Corvino A, Rosa D, Sbordone C, Nunziata A, Corvino F, Varelli C, et al. Diastasis of rectus abdominis muscles: patterns of anatomical variation as demonstrated by ultrasound. Pol J Radiol. 2019;84:e542-e8. Available from: https://doi.org/10.5114/pjr.2019.91303.
- Hernández-Gascón B, Mena A, Peña E, Pascual G, Bellón JM, Calvo B. Understanding the passive mechanical behavior of the human abdominal wall. Ann Biomed Eng. 2013;41(2):433-44. Available from: https://doi.org/10.1007/s10439-012-0672-7.
- Landon C, Crofts C, Smith A, Trowbridge E. Mechanical properties of fascia during pregnancy: a possible factor in the development of stress incontinence of urine. Contemp Rev Obstet Gynaecol. 1990;2:40-6.
- Beer GM, Schuster A, Seifert B, Manestar M, Mihic-Probst D, Weber SA. The normal width of the linea alba in nulliparous women. Clin Anat. 2009;22(6):706-11. Available from: https://doi.org/10.1002/ca.20836.
- Reinpold W, Köckerling F, Bittner R, Conze J, Fortelny R, Koch A, et al. Classification of Rectus Diastasis-A Proposal by the German Hernia Society (DHG) and the International Endohernia Society (IEHS). Front Surg. 2019;6:1. Available from: https://doi.org/10.3389/fsurg.2019.00001.
- Benjamin DR, Frawley HC, Shields N, van de Water ATM, Taylor NF. Relationship between diastasis of the rectus abdominis muscle (DRAM) and musculoskeletal dysfunctions, pain and quality of life: a systematic review. Physiotherapy. 2019;105(1):24-34. Available from: https://doi.org/10.1016/j.physio.2018.07.002.
- Crommert ME, Flink I, Gustavsson C. Predictors of Disability Attributed to Symptoms of Increased Interrecti Distance in Women after Childbirth: An Observational Study. Phys Ther. 2021;101(6). Available from: https://doi.org/10.1093/ptj/pzab064.
- Fuentes Aparicio L, Rejano-Campo M, Donnelly GM, Vicente-Campos V. Self-reported symptoms in women with diastasis rectus abdominis: A systematic review. J Gynecol Obstet Hum Reprod. 2020;50(7):101995. Available from: https://doi.org/10.1016/j.jogoh.2020.101995.
- SOReg. Annual report from SOReg 2019. Part 1 – surgical statistics and early complications.: Scandinavian Obesity Surgery Registry (SOReg); 2020. Årsrapporter volym 11:1. [accessed July 19 2021]. Available from: https://www.ucr.uu.se/soreg/component/edocman/soreg-annual-report-2019-part-1-2?Itemid=undefined.
- Turan V, Colluoglu C, Turkyilmaz E, Korucuoglu U. Prevalence of diastasis recti abdominis in the population of young multiparous adults in Turkey. Ginekol Pol. 2011;82(11):817-21.
- Nienhuijs SW, Berkvens EHM, de Vries Reilingh TS, Mommers EHH, Bouvy ND, Wegdam J. The male rectus diastasis: a different concept? Hernia. 2021. Available from: https://doi.org/10.1007/s10029-021-02467-9.
- Mota P, Pascoal AG, Carita AI, Bø K. Normal width of the inter-recti distance in pregnant and postpartum primiparous women. Musculoskelet Sci Pract. 2018;35:34-7. Available from: https://doi.org/10.1016/j.msksp.2018.02.004.
- Boissonnault JS, Blaschak MJ. Incidence of diastasis recti abdominis during the childbearing year. Phys Ther. 1988;68(7):1082-6. Available from: https://doi.org/10.1093/ptj/68.7.1082.
- Cavalli M, Aiolfi A, Bruni PG, Manfredini L, Lombardo F, Bonfanti MT, et al. Prevalence and risk factors for diastasis recti abdominis: a review and proposal of a new anatomical variation. Hernia. 2021;25(4):883-90. Available from: https://doi.org/10.1007/s10029-021-02468-8.
- Sperstad JB, Tennfjord MK, Hilde G, Ellström-Engh M, Bø K. Diastasis recti abdominis during pregnancy and 12 months after childbirth: prevalence, risk factors and report of lumbopelvic pain. Br J Sports Med. 2016;50(17):1092-6. Available from: https://doi.org/10.1136/bjsports-2016-096065.
- Statistiska Centralbyrån (SCB). Födda i Sverige. Uppdaterad 2021-03-24. [accessed July 21 2021]. Available from: https://www.scb.se/hitta-statistik/sverige-i-siffror/manniskorna-i-sverige/fodda-i-sverige/.
- Socialstyrelsen. Gravida och nyförlösta kvinnors situation och behov: En enkätundersökning och fokusgruppssamtal om hälsofrågor, oro, information, uppföljning och stöd. Stockholm: Socialstyrelsen; 2019. Artikelnummer 2019-11-6436. [accessed July 19 2021]. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2019-11-6436.pdf.
- Socialstyrelsen. Vård efter förlossning - En nationell kartläggning av vården till kvinnor efter förlossning. Stockholm: Socialstyrelsen; 2017. Artikelnummer 2017-4-13. [accessed July 19 2021]. Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/ovrigt/2017-4-13.pdf.
- SKR. Insatser för en stärkt eftervård – inom vårdkedjan för graviditet och förlossning. Stockholm: Sveriges kommuner och regioner (SKR); 2021. [accessed Mar 28 2021]. Available from: https://rapporter.skr.se/insatser-for-en-starkt-eftervard.html.
- Gustavsson C, Eriksson-Crommert M. Physiotherapists' and midwives' views of increased inter recti abdominis distance and its management in women after childbirth. BMC Womens Health. 2020;20(1):37. Available from: https://doi.org/10.1186/s12905-020-00907-9.
- van de Water AT, Benjamin DR. Measurement methods to assess diastasis of the rectus abdominis muscle (DRAM): A systematic review of their measurement properties and meta-analytic reliability generalisation. Man Ther. 2016;21:41-53. Available from: https://doi.org/10.1016/j.math.2015.09.013.
- Bursch SG. Interrater reliability of diastasis recti abdominis measurement. Phys Ther. 1987;67(7):1077-9. Available from: https://doi.org/10.1093/ptj/67.7.1077.
- Boxer S, Jones S. Intra-rater reliability of rectus abdominis diastasis measurement using dial calipers. Aust J Physiother. 1997;43(2):109-14. Available from: https://doi.org/10.1016/s0004-9514(14)60405-0.
- Emanuelsson P, Dahlstrand U, Strömsten U, Gunnarsson U, Strigård K, Stark B. Analysis of the abdominal musculo-aponeurotic anatomy in rectus diastasis: comparison of CT scanning and preoperative clinical assessment with direct measurement intraoperatively. Hernia. 2014;18(4):465-71. Available from: https://doi.org/10.1007/s10029-014-1221-0.
- Mendes Dde A, Nahas FX, Veiga DF, Mendes FV, Figueiras RG, Gomes HC, et al. Ultrasonography for measuring rectus abdominis muscles diastasis. Acta Cir Bras. 2007;22(3):182-6. Available from: https://doi.org/10.1590/s0102-86502007000300005.
- Elkhatib H, Buddhavarapu SR, Henna H, Kassem W. Abdominal musculoaponeuretic system: magnetic resonance imaging evaluation before and after vertical plication of rectus muscle diastasis in conjunction with lipoabdominoplasty. Plast Reconstr Surg. 2011;128(6):733e-40e. Available from: https://doi.org/10.1097/PRS.0b013e318230c8a1.
- Nahas FX, Augusto SM, Ghelfond C. Nylon versus polydioxanone in the correction of rectus diastasis. Plast Reconstr Surg. 2001;107(3):700-6. Available from: https://doi.org/10.1097/00006534-200103000-00008.
- Benjamin DR, van de Water AT, Peiris CL. Effects of exercise on diastasis of the rectus abdominis muscle in the antenatal and postnatal periods: a systematic review. Physiotherapy. 2014;100(1):1-8. Available from: https://doi.org/10.1016/j.physio.2013.08.005.
- Fernandes da Mota PG, Pascoal AG, Carita AI, Bo K. Prevalence and risk factors of diastasis recti abdominis from late pregnancy to 6 months postpartum, and relationship with lumbo-pelvic pain. Man Ther. 2015;20(1):200-5. Available from: https://doi.org/10.1016/j.math.2014.09.002.
- Keeler J, Albrecht M, Eberhardt L, Horn L, Donnelly C, Lowe D. Diastasis recti abdominis: a survey of women's health specialists for current physical therapy clinical practice for postpartum women. J Womens Health Phys Therap. 2012;36(3):131-42.
- Michalska A, Rokita W, Wolder D, Pogorzelska J, Kaczmarczyk K. Diastasis recti abdominis - a review of treatment methods. Ginekol Pol. 2018;89(2):97-101. Available from: https://doi.org/10.5603/GP.a2018.0016.
- Lee D, Hodges PW. Behavior of the Linea Alba During a Curl-up Task in Diastasis Rectus Abdominis: An Observational Study. J Orthop Sports Phys Ther. 2016;46(7):580-9. Available from: https://doi.org/10.2519/jospt.2016.6536.
- Werner LA, Dayan M. Diastasis Recti Abdominis-diagnosis, Risk Factors, Effect on Musculoskeletal Function, Framework for Treatment and Implications for the Pelvic Floor. Curr Womens Health Rev. 2019;15(2):86-101. Available from: https://doi.org/10.2174/1573404814666180222152952.
- Gluppe S, Engh ME, Bo K. What is the evidence for abdominal and pelvic floor muscle training to treat diastasis recti abdominis postpartum? A systematic review with meta-analysis. Braz J Phys Ther. 2021;25(6):664-75. Available from: https://doi.org/10.1016/j.bjpt.2021.06.006.
- Dufour S, Bernard S, Murray-Davis B, Graham N. Establishing expert-based recommendations for the conservative management of pregnancy-related diastasis rectus abdominis: a Delphi consensus study. J Womens Health Phys Therap. 2019;43(2):73-81.
- Pascoal AG, Dionisio S, Cordeiro F, Mota P. Inter-rectus distance in postpartum women can be reduced by isometric contraction of the abdominal muscles: a preliminary case-control study. Physiotherapy. 2014;100(4):344-8. Available from: https://doi.org/10.1016/j.physio.2013.11.006.
- Opala-Berdzik A, Dăbrowski S. Physiotherapy in diastasis of the rectus muscles of abdomen in women during pregnancy and postpartum. Physiotherapy/Fizjoterapia. 2009;17(4):4.
- Noble E. Essential Exercise for the Childbearing Year. 4th ed. Harwich, MA.: New Life Images; 2003.
- Jessen ML, Öberg S, Rosenberg J. Treatment Options for Abdominal Rectus Diastasis. Front Surg. 2019;6:65. Available from: https://doi.org/10.3389/fsurg.2019.00065.
- Eriksson Crommert M, Petrov Fieril K, Gustavsson C. Women's experiences of living with increased inter-recti distance after childbirth: an interview study. BMC Womens Health. 2020;20(1):260. Available from: https://doi.org/10.1186/s12905-020-01123-1.
- Hernández-Granados P, Henriksen NA, Berrevoet F, Cucurullo D, López-Cano M, Nienhuijs S, et al. European Hernia Society guidelines on management of rectus diastasis. Br J Surg. 2021. Available from: https://doi.org/10.1093/bjs/znab128.
- Carlstedt A, Bringman S, Egberth M, Emanuelsson P, Olsson A, Petersson U, et al. Management of Diastasis of the Rectus Abdominis Muscles: Recommendations for Swedish National Guidelines. Scand J Surg. 2020:1457496920961000. Available from: https://doi.org/10.1177/1457496920961000.
- Kvalitetsregistret för Svenska Bukväggsbråck. Årsrapport för 2019: Kvalitetsregistret för Svenska Bukväggsbråck; 2020. [accessed Aug 16 2021]. Available from: https://www.ventralhernia.se/files/2020-10/2020-svenska-bukvaggsbrack-arsrapport-2019.pdf.
- Carlstedt A, Pettersson U, Stark B, Strigard K. Abdominell rektusdiastas kan ge funktionella besvär - Indikation för behandling måste förtydligas. LAKARTIDNINGEN. 2018;115:FCL4.
- Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Bmj. 2009;339:b2535. Available from: https://doi.org/10.1136/bmj.b2535.
- SBU. Utvärdering av metoder i hälso- och sjukvården och insatser i socialtjänsten: en metodbok. Stockholm: Statens beredning för medicinsk och social utvärdering (SBU); 2020. [accessed May 20 2021]. Available from: https://www.sbu.se/metodbok.
- Gluppe SL, Hilde G, Tennfjord MK, Engh ME, Bo K. Effect of a Postpartum Training Program on the Prevalence of Diastasis Recti Abdominis in Postpartum Primiparous Women: A Randomized Controlled Trial. Phys Ther. 2018;98(4):260-8. Available from: https://doi.org/10.1093/ptj/pzy008.
- Tuttle LJ, Fasching J, Keller A, Patel M, Saville C, Schlaff R, et al. Noninvasive Treatment of Postpartum Diastasis Recti Abdominis: A Pilot Study. J Womens Health Phys Therap. 2018;42(2).
- Botla AMM, Saleh MSM. Effect of Russian current stimulation on abdominal strength and endurance in postnatal diastasis recti: A randomized controlled trial. Fizjoterapia Polska. 2020;20(1):16-22.
- Kamel DM, Yousif AM. Neuromuscular Electrical Stimulation and Strength Recovery of Postnatal Diastasis Recti Abdominis Muscles. Ann Rehabil Med. 2017;41(3):465-74. Available from: https://doi.org/10.5535/arm.2017.41.3.465.
- Emanuelsson P, Gunnarsson U, Strigård K, Stark B. Early complications, pain, and quality of life after reconstructive surgery for abdominal rectus muscle diastasis: a 3-month follow-up. J Plast Reconstr Aesthet Surg. 2014;67(8):1082-8. Available from: https://doi.org/10.1016/j.bjps.2014.04.015.
- Emanuelsson P, Gunnarsson U, Dahlstrand U, Strigård K, Stark B. Operative correction of abdominal rectus diastasis (ARD) reduces pain and improves abdominal wall muscle strength: A randomized, prospective trial comparing retromuscular mesh repair to double-row, self-retaining sutures. Surgery. 2016;160(5):1367-75. Available from: https://doi.org/10.1016/j.surg.2016.05.035.
- Swedenhammar E, Strigård K, Emanuelsson P, Gunnarsson U, Stark B. Long-term follow-up after surgical repair of abdominal rectus diastasis: a prospective randomized study. Scand J Surg. 2020:1457496920913677. Available from: https://doi.org/10.1177/1457496920913677.
- Keshwani N, Mathur S, McLean L. The impact of exercise therapy and abdominal binding in the management of diastasis recti abdominis in the early post-partum period: a pilot randomized controlled trial. Physiother Theory Pract. 2021;37(9):1018-33. Available from: https://doi.org/10.1080/09593985.2019.1675207.
- Thabet AA, Alshehri MA. Efficacy of deep core stability exercise program in postpartum women with diastasis recti abdominis: a randomised controlled trial. J Musculoskelet Neuronal Interact. 2019;19(1):62-8.
- Bobowik PŻ, Dąbek A. Physiotherapy in women with diastasis of the rectus abdominis muscles. Advances in Rehabilitation. 2018;32(3):11-7. Available from: https://doi.org/10.5114/areh.2018.80964.
- Laframboise FC, Schlaff RA, Baruth M. Postpartum Exercise Intervention Targeting Diastasis Recti Abdominis. Int J Exerc Sci. 2021;14(3):400-9.
- Camtö. Kirurgisk behandling av kvarstående abdominell rektusdiastas ett år efter förlossning. Region Örebro län: Centre for Assessment of Medical Technology in Örebro (Camtö); 2019. HTA-rapport 2019: 30. [accessed Nov 8 2021]. Available from: https://www.regionorebrolan.se/contentassets/a22815a843274fe8ac0172dc75319e42/rapporter-2019/2019.30-kirurgisk-behandling-av-kvarstaende-abdominell-rektusdiastas-1-ar-efter-forlossning.pdf
- Akram J, Matzen SH. Rectus abdominis diastasis. J Plast Surg Hand Surg. 2014;48(3):163-9. Available from: https://doi.org/10.3109/2000656x.2013.859145.
- Davenport MH, Ruchat SM, Sobierajski F, Poitras VJ, Gray CE, Yoo C, et al. Impact of prenatal exercise on maternal harms, labour and delivery outcomes: a systematic review and meta-analysis. Br J Sports Med. 2019;53(2):99-107. Available from: https://doi.org/10.1136/bjsports-2018-099821.
- ElHawary H, Abdelhamid K, Meng F, Janis JE. A Comprehensive, Evidence-Based Literature Review of the Surgical Treatment of Rectus Diastasis. Plast Reconstr Surg. 2020;146(5):1151-64. Available from: https://doi.org/10.1097/prs.0000000000007252.
- ElHawary H, Barone N, Zammit D, Janis JE. Closing the gap: evidence-based surgical treatment of rectus diastasis associated with abdominal wall hernias. Hernia. 2021;25(4):827-53. Available from: https://doi.org/10.1007/s10029-021-02460-2.
- Gormley J, Copeland A, Augustine H, Axelrod C, McRae M. Impact of Rectus Diastasis Repair on Abdominal Strength and Function: A Systematic Review. Cureus. 2020;12(12):e12358. Available from: https://doi.org/10.7759/cureus.12358.
- Gruszczyńska D, Truszczyńska-Baszak A. Exercises for pregnant and postpartum women with diastasis recti abdominis – literature review. Advances in Rehabilitation. 2018;32(3):27-35. Available from: https://doi.org/10.5114/areh.2018.80967.
- Hickey F, Finch JG, Khanna A. A systematic review on the outcomes of correction of diastasis of the recti. Hernia. 2011;15(6):607-14. Available from: https://doi.org/10.1007/s10029-011-0839-4.
- Jessen ML, Öberg S, Rosenberg J. Surgical techniques for repair of abdominal rectus diastasis: a scoping review. J Plast Surg Hand Surg. 2021;55(4):195-201. Available from: https://doi.org/10.1080/2000656x.2021.1873794.
- Malcher F, Lima DL, Lima R, Cavazzola LT, Claus C, Dong CT, et al. Endoscopic onlay repair for ventral hernia and rectus abdominis diastasis repair: Why so many different names for the same procedure? A qualitative systematic review. Surg Endosc. 2021;35(10):5414-21. Available from: https://doi.org/10.1007/s00464-021-08560-5.
- Mommers EHH, Ponten JEH, Al Omar AK, de Vries Reilingh TS, Bouvy ND, Nienhuijs SW. The general surgeon's perspective of rectus diastasis. A systematic review of treatment options. Surg Endosc. 2017;31(12):4934-49. Available from: https://doi.org/10.1007/s00464-017-5607-9.
- Olsson A, Kiwanuka O, Sandblom G, Stackelberg O. Evaluation of functional outcomes following rectus diastasis repair-an up-to-date literature review. Hernia. 2021;25(4):905-14. Available from: https://doi.org/10.1007/s10029-021-02462-0.
- Silecchia G, Campanile FC, Sanchez L, Ceccarelli G, Antinori A, Ansaloni L, et al. Laparoscopic ventral/incisional hernia repair: updated Consensus Development Conference based guidelines [corrected]. Surg Endosc. 2015;29(9):2463-84. Available from: https://doi.org/10.1007/s00464-015-4293-8.
- Van Kerckhoven L, Nevens T, Van De Winkel N, Miserez M, Vranckx JJ, Segers K. Treatment of rectus diastasis: should the midline always be reinforced with mesh? A systematic review. J Plast Reconstr Aesthet Surg. 2021;74(8):1870-80. Available from: https://doi.org/10.1016/j.bjps.2021.01.004.
- Yuan S, Li Y, Li Q, Fan L, Zhou J. Surgery Versus Non-surgery Interventions on Rectus Abdominis Diastasis With or Without Hernias: a Systematic Review. Indian J Surg. 2021. Available from: https://doi.org/10.1007/s12262-021-02792-4.
- Covidence systematic review software. Veritas Health Innovation, Melbourne, Australia. [accessed Nov 17 2021]. Available from: www.covidence.org.
- de Brito MJ, Nahas FX, Barbosa MV, Dini GM, Kimura AK, Farah AB, et al. Abdominoplasty and its effect on body image, self-esteem, and mental health. Ann Plast Surg. 2010;65(1):5-10. Available from: https://doi.org/10.1097/SAP.0b013e3181bc30f7.
- El-Mekawy HS, Eldeeb A, Lythy MAE, Elbegawy AF. Effect of Abdominal Exercises versus Abdominal Supporting Belt on Post-Partum Abdominal Efficiency and Rectus Separation. International Journal of Medical and Health Sciences. 2013;7:75-9. Available from: https://doi.org/10.5281/zenodo.1334606.
- Gama LJM, Barbosa MVJ, Czapkowski A, Ajzen S, Ferreira LM, Nahas FX. Single-Layer Plication for Repair of Diastasis Recti: The Most Rapid and Efficient Technique. Aesthet Surg J. 2017;37(6):698-705. Available from: https://doi.org/10.1093/asj/sjw263.
- Pawar PA, Yeole UL, Navale M, Patil K. Effect of kinesiotaping on diastasis recti in post-partum women. Indian J Public Health Res Dev. 2020;11(6):689-94.
- Serra-Renom JM, Martinez-Teixido L, Serra-Mestre JM. Abdominoplasty with Customized Transverse Musculoaponeurotic Plications. Plast Reconstr Surg. 2015;136(6):741e-9e. Available from: https://doi.org/10.1097/prs.0000000000001767.
- Staalesen T, Olsén MF, Elander A. The Effect of Abdominoplasty and Outcome of Rectus Fascia Plication on Health-Related Quality of Life in Post-Bariatric Surgery Patients. Plast Reconstr Surg. 2015;136(6):750e-61e. Available from: https://doi.org/10.1097/prs.0000000000001772.
- Wilhelmsson S, Fagevik Olsen M, Staalesen T, Elander A, Nygren-Bonnier M. Abdominal plasty with and without plication-effects on trunk muscles, lung function, and self-rated physical function. J Plast Surg Hand Surg. 2017;51(3):199-204. Available from: https://doi.org/10.1080/2000656X.2016.1222293.
- Deeks JJ, Higgins JPT, Altman DG. Chapter 10: Analysing data and undertaking meta-analyses. In: Cochrane Handbook for Systematic Reviews of Interventions. 6.2 ed: The Cochrane Collaboration; 2021. [accessed Dec 17 2021]. Available from: https://training.cochrane.org/handbook/current/chapter-10.
- Atkins D, Best D, Briss PA, Eccles M, Falck-Ytter Y, Flottorp S, et al. Grading quality of evidence and strength of recommendations. Bmj. 2004;328(7454):1490. Available from: https://doi.org/10.1136/bmj.328.7454.1490.
- Guyatt GH, Oxman AD, Vist GE, Kunz R, Falck-Ytter Y, Alonso-Coello P, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. Bmj. 2008;336(7650):924-6. Available from: https://doi.org/10.1136/bmj.39489.470347.AD.
- CCEMG - EPPI-Centre Cost Converter v.1.6. Eppi-Centre, London: The Cochrane and Campbell Economic Methods Group,. [updated 29 April 2019; accessed Nov 17 2021]. Available from: https://eppi.ioe.ac.uk/costconversion/default.aspx.
- Fysioterapeuterna. Lathund Nationella taxan 2021. Stockholm: Fysioterapeuterna; 2021. [accessed Mar 8 2021]. Available from: https://www.fysioterapeuterna.se/globalassets/foretagare/med-etablering/lathund-nationella-taxan-2021.pdf.
- Sjukvårdsregion Mellansverige. Regionala prislistan 2021. Sjukvårdsregion Mellansverige: Samverkansnämnden; 2020. [accessed Mar 8 2021]. Available from: https://www.xn–sjukvrdsregionmellan-0zb.se/samverkan/attachment/111.pdf.
- Sydöstra sjukvårdsregionen. Priser och ersättningar för Sydöstra sjukvårdsregionen 2021. Samverkansnämnden för sydöstra sjukvårdsregionen: Regionsjukvårdsstaben; 2020. Dnr: SVN 2020-54. [accessed Mar 8 2021]. Available from: https://sydostrasjukvardsregionen.se/wp-content/uploads/2020/11/SVN_20201127_punkt_5_2_priser_och_ersattningar_for_sydostra_sjukvardsregionen_2021.pdf.
- Södra regionvårdsnämnden. Regionala priser och ersättningar för södra sjukvårdsregionen. Lund: Södra regionvårdsnämnden; 2020. [accessed Mar 8 2021]. Available from: https://sodrasjukvardsregionen.se/download/regionala-priser-och-ersattningar-for-sodra-sjukvardsregionen-2021/?wpdmdl=21717&masterkey=601157116d92d.
- Västra sjukvårdsregionen. Utomlänspriser 2021. För vårdtjänster enligt samverkansavtal om hälso- och sjukvård inom Västra sjukvårdsregionen. Västra sjukvårdsregionen: Samverkansnämnden; 2021. [accessed Mar 8 2021]. Available from: https://alfresco-offentlig.vgregion.se/alfresco/service/vgr/storage/node/content/workspace/SpacesStore/53283308-2854-48cc-916c-d4ddade5ddd7/Utoml%c3%a4nspriser%20V%c3%a4stra%20sjukv%c3%a5rdsregionen%202021.pdf?a=false&guest=true.
- Samverkansnämnden Stockholm - Gotland. Utomlänsprislista år 2021. Region Stockholm - Region Gotland. Pislista övrig öppen vård. Gäller från 1 januari 2021 - 31 december 2021. Samverkansnämnden Stockholm - Gotland; 2021. [accessed Mar 8 2021]. Available from: https://www.sll.se/globalassets/5.-politik/politiska-organ/samverkansnamnden-sthlm-gotland/2021/prislistor-2021/bilaga-5-ovrig-oppenvard-2021.pdf.
- Prislistor norra sjukvårdsregionen. Regional prislista för Norra sjukvårdsregionens länssjukvård och primärvård, 2021 - bilaga 3 (utgåva 2). Umeå: Norra sjukvårdsregionförbundet,. [accessed Mar 8 2021]. Available from: https://www.norrlandstingen.se/halso-och-sjukvard/avtal-och-priser/prislistor-norra-sjukvardsregionen/.
- KPP-databas för somatisk vård. Sveriges kommuner och regioner. [accessed 2021-03-08]. Available from: https://statva.skl.se/KPP_somatik_publik.html.
- Socialstyrelsen. Ändringar i och tillägg till tryckt Internationell statistisk klassifikation av sjukdomar och relaterade hälsoproblem - systematisk förteckning (ICD-10-SE). Stockholm: Socialstyrelsen; 2020. [accessed Nov 12 2020]. Available from: https://www.socialstyrelsen.se/utveckla-verksamhet/e-halsa/klassificering-och-koder/senaste-uppdateringar/.
- SKR. Nationella KPP-principer. Version 4. Kostnad per patient. Stockholm: Sveriges kommuner och regioner (SKR); 2020. [accessed Mar 8 2021]. Available from: https://webbutik.skr.se/bilder/artiklar/pdf/7585-881-4.pdf?issuusl=ignore.
- SBU. Etiska aspekter på insatser inom hälso- och sjukvården. En vägledning för att identifiera relevanta etiska aspekter. Stockholm: Statens beredning för medicinsk och social utvärdering (SBU); 2021. [accessed Dec 01 2021]. Available from: https://www.sbu.se/globalassets/ebm/etiska_aspekter_halso_sjukvarden.pdf.
- The HTAi Interest Group for Patient and Citizen Involvement in HTA (PCIG). Health technology assessment international (HTAi). [accessed Dec 1 2021]. Available from: https://htai.org/interest-groups/pcig/.
- Barber MD, Walters MD, Bump RC. Short forms of two condition-specific quality-of-life questionnaires for women with pelvic floor disorders (PFDI-20 and PFIQ-7). Am J Obstet Gynecol. 2005;193(1):103-13. Available from: https://doi.org/10.1016/j.ajog.2004.12.025.
- Avalos L, Tylka TL, Wood-Barcalow N. The Body Appreciation Scale: development and psychometric evaluation. Body Image. 2005;2(3):285-97. Available from: https://doi.org/10.1016/j.bodyim.2005.06.002.
- Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine (Phila Pa 1976). 1983;8(2):141-4. Available from: https://doi.org/10.1097/00007632-198303000-00004.
- Clay L, Fränneby U, Sandblom G, Gunnarsson U, Strigård K. Validation of a questionnaire for the assessment of pain following ventral hernia repair – the VHPQ. Langenbecks Arch Surg. 2012;397(8):1219-24. Available from: https://doi.org/10.1007/s00423-012-0932-x.
- Metodrådet i Sydöstra sjukvårdsregionen. Vetenskaplig evidens för behandling av abdominell rektusmuskeldiastas (ARD). Region Jönköpings län: Sydöstra sjukvårdsregionen; 2017. [accessed Sep 6 2021]. Available from: https://plus.rjl.se/info_files/infosida40495/metodraadet_so_ard_2017_09_06.pdf.
- Sammanräknad förvärvsinkomst för boende i Sverige hela året efter region, kön, ålder och inkomstklass. År 1999-2019. Statistikmyndigheten (SCB). [accessed 2021-08-26]. Available from: http://www.statistikdatabasen.scb.se/pxweb/sv/ssd/START__HE__HE0110__HE0110A/SamForvInk1/#.
- Skatteverket. Arbetsgivaravgifter. Skatteverket; 2020. [accessed Aug 26 2021]. Available from: https://www.skatteverket.se/foretag/arbetsgivare/arbetsgivaravgifterochskatteavdrag/arbetsgivaravgifter.4.233f91f71260075abe8800020817.html.
- Sociala avgifter. Stockholm: Ekonomifakta. [updated Sep 21 2021; accessed Nov 17 2021]. Available from: https://www.ekonomifakta.se/fakta/skatter/skatt-pa-arbete/sociala-avgifter/.
- SOU 1995:5. Vårdens svåra val. Statens offentliga utredningar. Stockholm. [updated April 2 2015; accessed Dec 16 2021]. Available from: https://www.regeringen.se/49b6ca/contentassets/6c4cb9f4c3ef4296b68ea7c6cefbf1d2/del-1-kap.-1-t.o.m.-kap.-8-vardens-svara-val.
- Olsson A, Kiwanuka O, Wilhelmsson S, Sandblom G, Stackelberg O. Cohort study of the effect of surgical repair of symptomatic diastasis recti abdominis on abdominal trunk function and quality of life. BJS Open. 2019;3(6):750-8. Available from: https://doi.org/10.1002/bjs5.50213.
- Olsson A, Kiwanuka O, Wilhelmsson S, Sandblom G, Stackelberg O. Surgical repair of diastasis recti abdominis provides long-term improvement of abdominal core function and quality of life: a 3-year follow-up. BJS Open. 2021;5(5). Available from: https://doi.org/10.1093/bjsopen/zrab085.
- Ranney B. Diastasis recti and umbilical hernia causes, recognition and repair. S D J Med. 1990;43(10):5-8.
- Brazier JE, Harper R, Jones NM, Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 health survey questionnaire: new outcome measure for primary care. British Medical Journal. 1992;305(6846):160. Available from: https://doi.org/10.1136/bmj.305.6846.160.
- Biörserud C, Olbers T, Fagevik Olsén M. Patients' experience of surplus skin after laparoscopic gastric bypass. Obes Surg. 2011;21(3):273-7. Available from: https://doi.org/10.1007/s11695-009-9849-z.
- Staalesen T, Olsén MF, Elander A. Complications of abdominoplasty after weight loss as a result of bariatric surgery or dieting/postpregnancy. J Plast Surg Hand Surg. 2012;46(6):416-20. Available from: https://doi.org/10.3109/2000656x.2012.717898.
- Depledge J, McNair P, Ellis R. Exercises, Tubigrip and taping: can they reduce rectus abdominis diastasis measured three weeks post-partum? Musculoskeletal Science and Practice. 2021;53:102381. Available from: https://doi.org/10.1016/j.msksp.2021.102381.
- Gluppe SB, Engh ME, Bø K. Immediate Effect of Abdominal and Pelvic Floor Muscle Exercises on Interrecti Distance in Women With Diastasis Recti Abdominis Who Were Parous. Phys Ther. 2020;100(8):1372-83. Available from: https://doi.org/10.1093/ptj/pzaa070.