Rehabilitation for adults with traumatic brain injury
A systematic review and assessment of medical, economic, social and ethical aspects
Executive summary
 Share on Facebook
Share on Facebook
 Share on LinkedIn
Share on LinkedIn
 Share via Email
Share via Email
Conclusions
Rehabilitation for persons with mild traumatic brain injury (TBI) and persistent post-concussion symptoms:
- Specialised brain injury rehabilitation that employs problem-solving therapy or cognitive behavioural therapy (CBT) results in less severe post-concussion symptoms and depressive symptoms, improved psychological function, increased activity and participation and quality of life, when compared to usual care (low certainty of evidence, ⊕⊕◯◯). A simple cost-effectiveness analysis indicates a cost of about 500 000 SEK per quality-adjusted life year (QALY) for the intervention, but this cost might be overestimated since it does not incorporate possible cost savings resulting from the rehabilitation.
- Specialised interdisciplinary brain injury rehabilitation results in reduced post-concussion symptoms, when compared to usual care (low certainty of evidence, ⊕⊕◯◯).
Rehabilitation for persons with moderate to severe TBI:
- As few high-quality studies were identified, it was not possible to estimate the effects of vocational rehabilitation, rehabilitation with case management/coordinator, rehabilitation in supported living, specialised inpatient rehabilitation or specialised outpatient rehabilitation (very low certainty of evidence, ⊕◯◯◯).
Experiences and perspectives of the rehabilitation process from persons with TBI:
- A synthesis of qualitative studies showed that the persons with TBI were struggling on their own with adapting in their daily lives and that family members were important in that process. They experienced limited access to rehabilitation services, and perceived the interventions they receive as neither individualised nor coordinated. Furthermore, they experienced professional and respectful treatment, as well as individualised information, as beneficial for their rehabilitation process.
Current state of research in the field:
- There is a general need for high-quality studies with control groups in this research field. Standardization of study design, treatment intensity, as well as outcome instruments and measures is needed to allow the effects of different forms of rehabilitation to be compared. It would be preferable if future studies assess the effects and costs of interventions beyond one year. Furthermore, there is a need for studies in settings directly relevant to the Swedish health care system that investigate intervention efficacity as well as individuals’ experiences of receiving rehabilitation.
Aim
The aim of the project was to assess rehabilitation interventions for adults with traumatic brain injury from medical, social, ethical and health economic perspectives.
Background
Traumatic brain injuries (TBIs) are caused by external force or sudden movement of the head. The most common causes are falls and traffic accidents. The injuries are classified as mild, moderate or severe, based on the duration of unconsciousness and the extent of posttraumatic amnesia. TBI is the most common cause of neurological disability and has often a major impact on life for the affected persons and their family members. According to Swedish hospital data, approximately 10 000 cases are treated in inpatient care and 20 000 in outpatient care every year. Approximately 50% of TBI patients are 65 years or older.
Most persons with mild TBI (including concussions) experience full recovery within a few weeks, but up to 20% experience persistent symptoms including fatigue, headache, hypersensitivity to visual and auditory stimuli, dizziness and memory problems. Access to rehabilitation services for this group varies in Sweden, from specialised care to limited care or no interventions at all.
Persons with moderate to severe TBI typically receive individual rehabilitation from a specialised inpatient brain injury team, but rehabilitation can also take place within geriatric care. After discharge from hospital, rehabilitation is given in outpatient care according to local routines.
Method
Systematic literature reviews were conducted in accordance with PRISMA guidelines and SBU’s standardised methods. All steps in the literature assessment were conducted by two independent reviewers, and any disagreement was resolved by discussion. Quantitative data were combined in meta-analyses when study characteristics and outcome measures were comparable. The findings from the qualitative studies were synthesised through an inductive content analysis. The certainty of evidence of quantitative results was assessed according to grading of recommendations assessment, development and evaluation (GRADE), and qualitative results were assessed with Confidence in Evidence from Reviews of Qualitative research (CERQual).
Inclusion Criteria
Quantitative studies
Population:
Adults (≥16 years old) with traumatic brain injury (TBI). Studies with mixed populations were accepted if the proportion of TBI patients comprised >50%.
Interventions (1-6):
- Specialised inpatient rehabilitation at an early stage after injury for patients with moderate to severe TBI
- Specialised outpatient rehabilitation at a later stage after injury for patients with moderate to severe TBI
- Specialised outpatient rehabilitation for patients with mild TBI and persistent residual symptoms
- Rehabilitation with case management or coordinator
- Supported living in residential homes
- Vocational rehabilitation
Comparisons (1-6):
- Less specialised rehabilitation or no rehabilitation
- Less specialised rehabilitation or no rehabilitation
- Less specialised rehabilitation or no rehabilitation
- Rehabilitation without case manager
- Living at home or other forms of living
- Other forms of rehabilitation or no rehabilitation
Outcome:
- Function
- Activity and participation
- Quality of life
- Mortality
Health economic studies
Population, Interventions, and Comparison: Same as for quantitative studies
Outcome: Resource use, costs and cost-effectiveness
Qualitative studies
Population: Same as for quantitative studies
Phenomena of Interest: Experiences of the rehabilitation process and health care contacts
Context: Hospital and at home
Study design
Quantitative studies: Randomised controlled trials (RCT) or non-randomised controlled studies of interventions (NRSI).
Health economic studies: Relevant study designs included cost studies, comparative studies of resource use, and economic evaluations, including modelling studies.
Qualitative studies: Studies with qualitative design exploring patients’ experiences and perspectives
Systematic reviews were included if inclusion and exclusion criteria were matched by our stated criteria.
Language: English, Swedish, Norwegian, or Danish.
Search period: From 1990 or 2000 (depending on intervention) and onwards. Final search: March 2019.
Databases searched: Cochrane Controlled Register of Trials (Central), PubMed (NLM), EMBASE (Elsevier), CINAHL (EBSCO), PsycINFO (EBSCO), SocINDEX.
Client/patients involvement: Yes
Results
In total, 19 RCTs, 12 NRSIs, 10 qualitative and 3 health economic studies were included in the report (see flow charts).
Effects of the rehabilitation interventions
The results from the quantitative studies assessing the interventions’ effects on health and quality of life are summarised in Table 2. The six initial research questions resulted in 15 unique comparisons. Results favouring the intervention group were seen from specialized brain injury rehabilitation for persons with persistent post-concussion symptoms after mild TBI, when compared to usual care (low certainty of evidence). For all other comparisons, the results had very low certainty of evidence, which means that it was not possible to assess the effects of these interventions.
Health economic assessment
The systematic literature review resulted in three studies that fulfilled the eligibility and quality criteria; these studies only addressed partial aspects of the research questions. A study from the US compared telephone-based problem-solving therapy to usual care in a military health care setting. A Dutch study analysed costs for supported living one year before and one year after the intervention. Finally, an economic evaluation from the UK compared specialised vocational rehabilitation to usual care.
A simple cost-effectiveness analysis was conducted for specialized brain injury rehabilitation consisting of telephone-based problem-solving therapy, which resulted in a cost of around 500 000 SEK per QALY. It is possible that the costs are overestimated, since the calculation does not incorporate possible cost savings resulting from the rehabilitation. Whether or not the intervention should be considered cost-effective depends on what cost decision-makers deem appropriate in relation to the effect in this particular patient population.
Experiences and perspectives on the rehabilitation
The systematic review of qualitative research resulted in 10 studies, for which the findings were synthesised into three main categories. The synthesis showed that the persons with TBI were struggling on their own with adapting in their daily lives and that family members were important in that process. They experienced limited access to rehabilitation services, and perceived the interventions they received as neither individualised nor coordinated. Furthermore, they experienced professional and respectful treatment, as well as individualised information, as beneficial for their rehabilitation process.
Table 1. Overview of findings regarding the effects of the interventions. Only main groups of outcomes are shown. All results with low certainty of evidence were in favour of the intervention.
| Research question | Intervention | Comparison | Outcome (certainty of evidence) | |||
| Function | Activity and participation | Quality of life | Mortality | |||
| CBT = Cognitive behavioural therapy, VR = Vocational rehabilitation | ||||||
| Specialised inpatient rehabilitation, moderate to severe TBI | Specialised inpatient rehabilitation | Less specialised rehabilitation | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies |
| Specialised outpatient rehabilitation, moderate to severe TBI | CBT | Usual care | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies | No studies |
| Multidisciplinary outpatient rehabilitation | Usual care | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies | |
| Specialised outpatient rehabilitation, mild TBI | CBT or problem-solving therapy | Usual care | Low ⊕⊕◯◯ | Low ⊕⊕◯◯ | Low ⊕⊕◯◯ | No studies |
| CBT | Counselling | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies | No studies | |
| Interdisciplinary rehabilitation | Usual care | Low ⊕⊕◯◯ | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies | |
| Rehabilitation with coordinator | Case management | Without case management | No studies | Very low ⊕◯◯◯ | No studies | No studies |
| Peer mentoring | Without peer mentoring | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies | |
| Resource facilitation | Without resource facilitation | No studies | Very low ⊕◯◯◯ | No studies | No studies | |
| Supported living | Residential living + rehabilitation | Living at home + rehabilitation | No studies | Very low ⊕◯◯◯ | No studies | No studies |
| Transitional living + rehabilitation | Living at home + rehabilitation | No studies | Very low ⊕◯◯◯ | No studies | No studies | |
| Vocational rehabilitation (VR) | Virtual reality-based VR | Psychoeducation | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies | No studies |
| Individual VR | VR in groups | No studies | Very low ⊕◯◯◯ | No studies | No studies | |
| Goal-directed, environmentfocused outpatient VR | Goal-directed, environmentfocused homebased VR | No studies | Very low ⊕◯◯◯ | No studies | No studies | |
| Specialised VR | Usual care | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | Very low ⊕◯◯◯ | No studies | |
Ethical and societal aspects
Persons with traumatic brain injury may have impaired capacity to make informed decisions and to make their own voice heard. This means that their autonomy is reduced, and they may be dependent on the help from family members or health care staff. Unstructured care pathways involving many different care givers in combination with the individuals’ complex rehabilitation needs and vulnerable situation, amplifies the importance of adequate support, information and coordination.
It is necessary for the health care system to provide various forms of rehabilitation interventions in order to meet patients’ individual needs. More research is needed, however, in order to conclude on which interventions that are the most effective, and in order to make health economic assessments preceding priority decisions.
It is important to acknowledge aspects related to equity and justice regarding the distribution of rehabilitation interventions, where the patient’s geographical residence, age and ability to work may impact on the access to rehabilitation. Presence or absence of family members may also have influence on the patient’s access to support and services.
Discussion
It should be noted that very low certainty of evidence does not imply that an intervention lacks effect, but rather that its effect has not been sufficiently researched. This assessment has identified several scientific knowledge gaps where there is a substantial need for further research. As there was an extensive heterogeneity across the included studies regarding design, treatment intensity, outcomes and instruments, it is desirable for the field to strive for improved consistency in design and reporting.
It is also important to acknowledge that the assessment did not target rehabilitation interventions that focus on treating single symptoms. Therefore, there are several rehabilitation forms that are not included in the report.
The full report in Swedish
The full report "Rehabilitering för vuxna med traumatisk hjärnskada" (in Swedish)
Scientific article
Moller MC, Lexell J, Wilbe Ramsay K. Effectiveness of specialized rehabilitation after mild traumatic brain injury: A systematic review and meta-analysis. Journal of rehabilitation medicine : official journal of the UEMS European Board of Physical and Rehabilitation Medicine. 2021;53(2):jrm00149. Read abstract
Project group
Experts
- Lina Bunketorp Käll, Sahlgrenska University Hospital, Gothenburg, Sweden
- Jan Lexell, Uppsala University, Sweden
- Maria Larsson Lund, Luleå University, Sweden
- Marika Möller, Danderyd University Hospital, Stockholm, Sweden
- Maud Stenberg, Norrland University Hospital, Umeå, Sweden
- Thomas Strandberg, University of Örebro, Sweden
SBU
- Karin Wilbe Ramsay, Project Manager, karin.wilberamsay@sbu.se
- Agneta Pettersson, Assistant Project Manager
- Ann Kristine Jonsson, Information Specialist
- Elisabeth Gustafsson, Project Administrator
- Jenny Berg, Health Economist (from May 2019)
- Naama Kenan Modén, Assistant Project Manager
- Pia Johansson, Health Economist (to April 20)
Internal Reviewer from SBU´s Scientific Advisory Board
Britt-Marie Stålnacke, Umeå University, Sweden
External Reviewers
- Cecilie Røe, Oslo University Hospital, Norway
- Gunilla Eriksson, Uppsala University, Sweden
- Olli Tenovuo, Turku University Hospital, Finland
English proofreading
Rebecca Silverstein, SBU
Flow charts of included studies
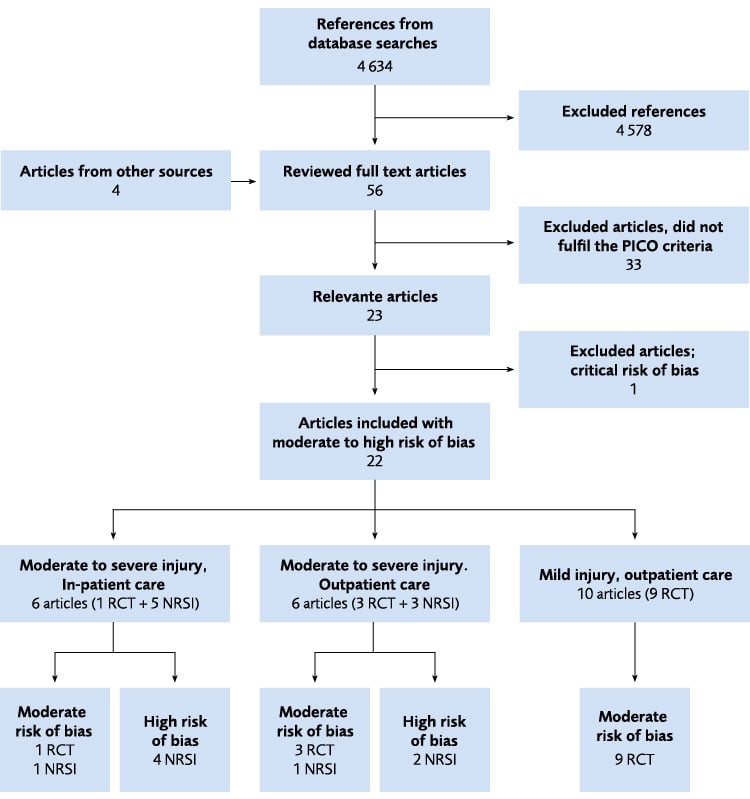
Figure 4 Flow chart of the literature review for the three research questions relating to specialised brain injury rehabilitation compared to less specialised interventions. A common literature search was made for the three research questions. Two of the included articles contained data from the same randomised study. Studies with critical risk of bias were excluded. NRSI = Non-randomised study of intervention; RCT = Randomised controlled trial.
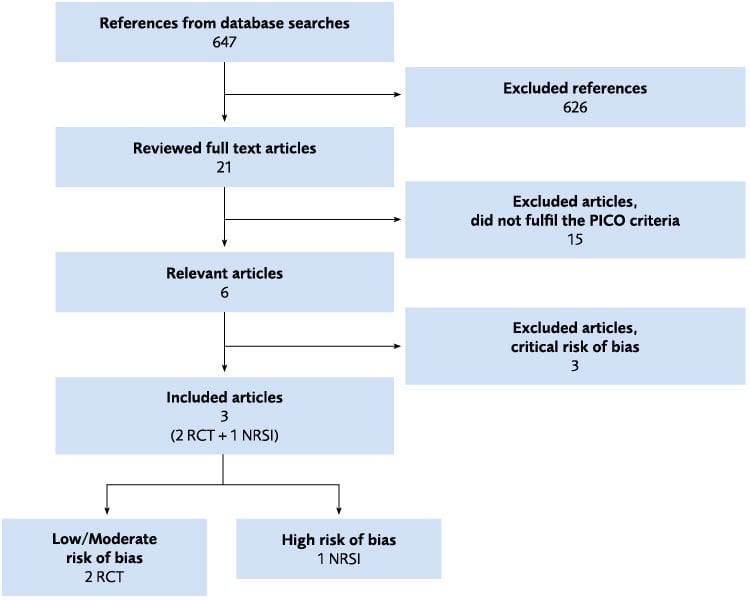
Figure 4.16 Flow chart of the literature review regarding Coordinator or Case management. NRSI = Non-randomised study of intervention; RCT = Randomised controlled trial.
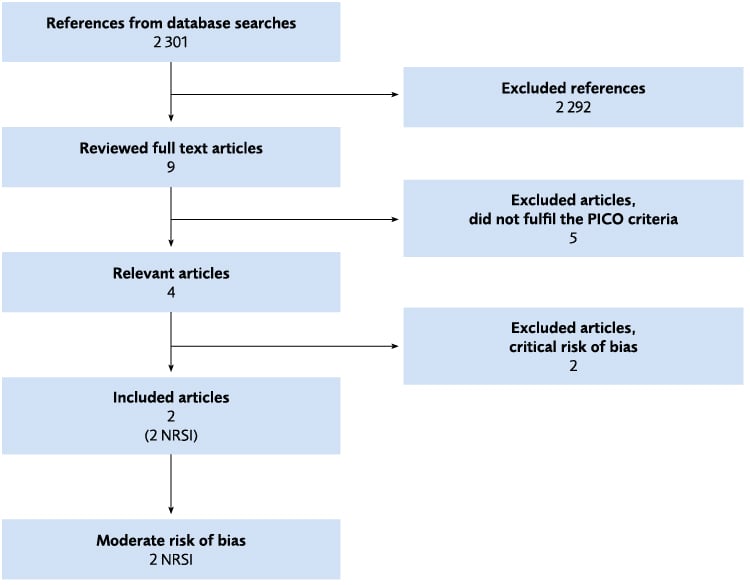
Figure 4.17 Flow chart of the literature review regarding rehabilitation in supported living. NRSI = Non-randomised study of intervention; RCT = Randomised controlled trial.
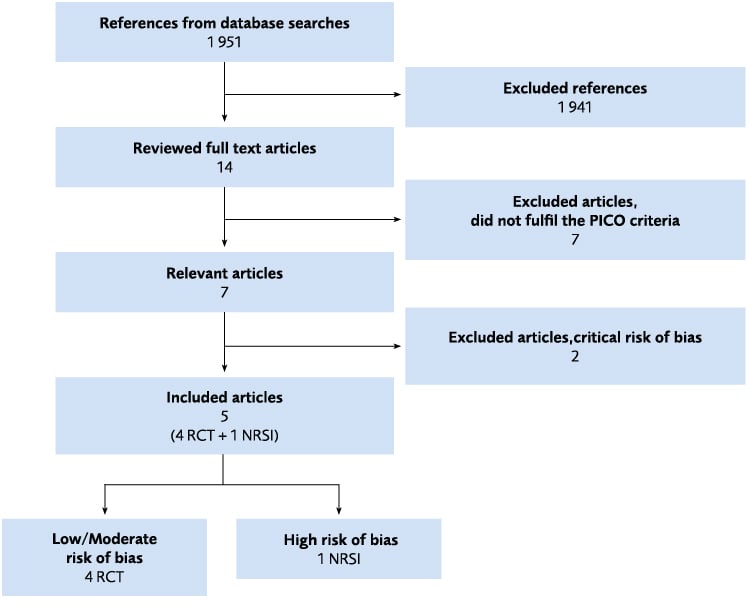
Figure 4.18 Flow chart of the literature review regarding vocational rehabilitation. NRSI = Non-randomised study of intervention; RCT = Randomised controlled trial.
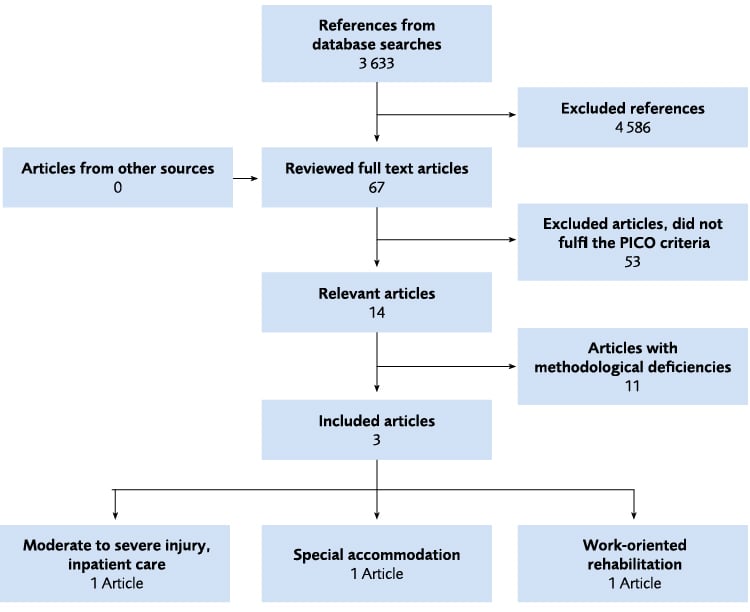
Figure 5.1 Flow chart of the Health economic literature review.
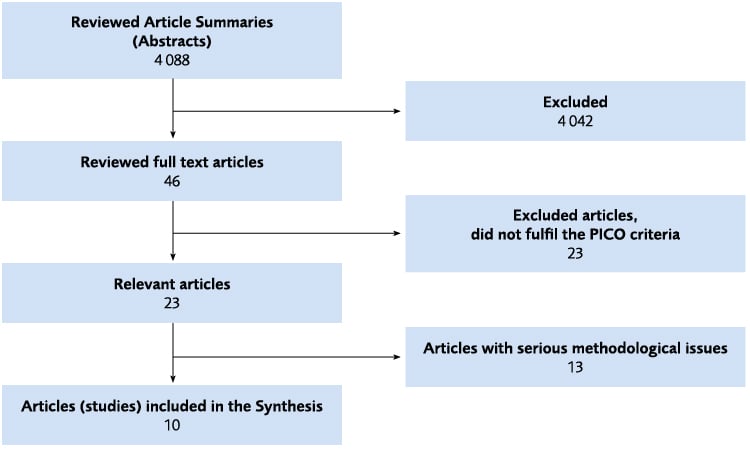
Figure 6.1 Flow chart of the literature review on the intervention Experiences and perceptions of rehabilitation.
References
- Socialstyrelsen. Rehabilitering för personer med traumatisk hjärnskada. Landstingens rehabiliteringsinsatser. Artikelnr 2012-12-27 [Internet]. Nedladdad 190709.
- Turner-Stokes L, Pick A, Nair A, Disler PB, Wade DT. Multi-disciplinary rehabilitation for acquired brain injury in adults of working age. Cochrane Database Syst Rev 2015:Cd004170.
- Kumar KS, Samuelkamaleshkumar S, Viswanathan A, Macaden AS. Cognitive rehabilitation for adults with traumatic brain injury to improve occupational outcomes. Cochrane Database Syst Rev 2017;6:Cd007935.
- Linden M, Hawley C, Blackwood B, Evans J, Anderson V, O'Rourke C. Technological aids for the rehabilitation of memory and executive functioning in children and adolescents with acquired brain injury. Cochrane Database Syst Rev 2016;7:Cd011020.
- Styrke J, Stalnacke BM, Sojka P, Bjornstig U. Traumatic brain injuries in a well-defined population: epidemiological aspects and severity. J Neurotrauma 2007;24:1425-36.
- Godbolt AK, Deboussard CN, Stenberg M, Lindgren M, Ulfarsson T, Borg J. Disorders of consciousness after severe traumatic brain injury: a Swedish-Icelandic study of incidence, outcomes and implications for optimizing care pathways. J Rehabil Med 2013;45:741-8.
- Thurman DJ, Alverson C, Dunn KA, Guerrero J, Sniezek JE. Traumatic brain injury in the United States: A public health perspective. J Head Trauma Rehabil 1999;14:602-15.
- Tagliaferri F, Compagnone C, Korsic M, Servadei F, Kraus J. A systematic review of brain injury epidemiology in Europe. Acta Neurochir (Wien) 2006;148:255-68; discussion 268.
- Bener A, Omar AO, Ahmad AE, Al-Mulla FH, Abdul Rahman YS. The pattern of traumatic brain injuries: a country undergoing rapid development. Brain Inj 2010;24:74-80.
- Fleming J, Sampson J, Cornwell P, Turner B, Griffin J. Brain injury rehabilitation: the lived experience of inpatients and their family caregivers. Scand J Occup Ther 2012;19:184-93.
- Jumisko E, Lexell J, Soderberg S. Living with moderate or severe traumatic brain injury: the meaning of family members' experiences. J Fam Nurs 2007;13:353–69.
- Teasdale G, Jennett B. Assessment of coma and impaired consciousness. A practical scale. Lancet 1974;2:81-4.
- Starmark JE, Stalhammar D, Holmgren E, Rosander B. A comparison of the Glasgow Coma Scale and the Reaction Level Scale (RLS85). J Neurosurg 1988;69:699-706.
- A FK, A DS, F LH, Suzanne P, L vdBC, Korné J, et al. Risk of Intracranial Complications in Minor Head Injury: The Role of Loss of Consciousness and Post-Traumatic Amnesia in a Multi-Center Observational Study. Journal of Neurotrauma 2019;36:2377-384.
- ACRM. Mild traumatic Brain Injury Committee of the American Congress of Rehabilitation Medicine. [Internet] Tillgänglig från: https://acrm.org/wp-content/uploads/pdf/TBIDef_English_10-10.pdf. Nedladdad: 1907081993
- Mayer AR, Quinn DK, Master CL. The spectrum of mild traumatic brain injury: A review. Neurology 2017;89:623-32.
- Lannsjo M, Backheden M, Johansson U, Af Geijerstam JL, Borg J. Does head CT scan pathology predict outcome after mild traumatic brain injury? Eur J Neurol 2013;20:124-9.
- Stålnacke B. Community integration, social support and life satisfaction in relation to symptoms 3 years after mild traumatic brain injury. Brain Injury 2007;21:933-42.
- Stålnacke B, Björnstig U, Karlsson K, Sojka P. One-year follow-up of mild traumatic brain injury: post-concussion symptoms, disabilities and life satisfaction in relation to serum levels of S-100B and neurone-specific enolase in acute phase. J Rehabil Med (Taylor & Francis Ltd) 2005;37:300-305.
- McMahon P, Hricik A, Yue JK, Puccio AM, Inoue T, Lingsma HF, et al. Symptomatology and functional outcome in mild traumatic brain injury: results from the prospective TRACK-TBI study. J Neurotrauma 2014;31:26-33.
- af Geijerstam JL, Britton M. Mild head injury – mortality and complication rate: meta-analysis of findings in a systematic literature review. Acta Neurochir (Wien) 2003;145:843-50; discussion 850.
- Madsen T, Erlangsen A, Orlovska S, Mofaddy R, Nordentoft M, Benros ME. Association Between Traumatic Brain Injury and Risk of Suicide. JAMA 2018;320:580-88.
- af Geijerstam JL, Oredsson S, Britton M. Medical outcome after immediate computed tomography or admission for observation in patients with mild head injury: randomised controlled trial. Bmj 2006;333:465.
- Stulemeijer M, van der Werf S, Borm GF, Vos PE. Early prediction of favourable recovery 6 months after mild traumatic brain injury. J Neurol Neurosurg Psychiatry 2008;79:936-42.
- Levin HS, Diaz-Arrastia RR. Diagnosis, prognosis, and clinical management of mild traumatic brain injury. Lancet Neurology 2015;14:506-17.
- Whitnall L, McMillan TM, Murray GD, Teasdale GM. Disability in young people and adults after head injury: 5–7 year follow up of a prospective cohort study. J Neurol Neurosurg Psychiatry 2006;77:640-45.
- Godbolt AK, Cancelliere C, Hincapie CA, Marras C, Boyle E, Kristman VL, et al. Systematic review of the risk of dementia and chronic cognitive impairment after mild traumatic brain injury: results of the International Collaboration on Mild Traumatic Brain Injury Prognosis. Arch Phys Med Rehabil 2014;95:S245-56.
- Giacino JT, Katz DI, Schiff ND, Whyte J, Ashman EJ, Ashwal S, et al. Comprehensive Systematic Review Update Summary: Disorders of Consciousness: Report of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology; the American Congress of Rehabilitation Medicine; and the National Institute on Disability, Independent Living, and Rehabilitation Research. Arch Phys Med Rehabil 2018;99:1710-19.
- Socialstyrelsen. Statistikdatabasen. [Internet] Tillgänglig från: https://www.socialstyrelsen.se/statistik-och-data/statistik/statistikdatabasen/ Nedladdad 190807.
- Zasler ND. Brain Injury Medicine. Principles and Practice. Seond ed, Demos Medical Publishing; 2002; ISSN: 9781936287277.
- WHO. International Classification of Diseases. [Internet] Tillgänglig från: https://www.who.int/classifications/icd/en/ Nedladdad 20190907.
- Gardner RC, Yaffe K. Epidemiology of mild traumatic brain injury and neurodegenerative disease. Mol Cell Neurosci 2015;66:75-80.
- Jackson H, Philp E, Nuttall RL, Diller L. Traumatic brain injury: A hidden consequence for battered women. Prof Psychol Res Pr 2002;33:39-45.
- Cassidy JD, Carroll LJ, Peloso PM, Borg J, von Holst H, Holm L, et al. Incidence, risk factors and prevention of mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med 2004:28-60.
- Borg J, Roe C, Nordenbo A, Andelic N, de Boussard C, af Geijerstam JL. Trends and challenges in the early rehabilitation of patients with traumatic brain injury: a Scandinavian perspective. Am J Phys Med Rehabil 2011;90:65-73.
- Pedersen K, Fahlstedt M, Jacobsson A, Kleiven S, von Holst H. A National Survey of Traumatic Brain Injuries Admitted to Hospitals in Sweden from 1987 to 2010. Neuroepidemiology 2015;45:20-7.
- Unden J, Ingebrigtsen T, Romner B. Scandinavian guidelines for initial management of minimal, mild and moderate head injuries in adults: an evidence and consensus-based update. BMC Med 2013;11:50.
- Burns Jr J, Hauser WA. The Epidemiology of Traumatic Brain Injury: A Review. Epilepsia 2003;44:2-10.
- Roozenbeek B, Maas AI, Menon DK. Changing patterns in the epidemiology of traumatic brain injury. Nat Rev Neurol 2013;9:231-6.
- von Wild KRH. Posttraumatic rehabilitation and one year outcome following acute traumatic brain injury (TBI): Data from the well defined population based German Prospective Study 2000–2002. In; 2008; Vienna: Springer Vienna; 2008. p 55-60.
- Lexell J. Rehabilitation of traumatic brain injuries in Sweden. J Head Trauma Rehabil 2007;22:229-33.
- Undén J, Bellander BM, Romner B. Uppdaterad handläggning av vuxna med skallskada. SNC:s nya riktlinjer ger vägledning vid minimal, lätt och medelsvår skada. Läkartidningen 2013;110:1868-69.
- Bellander BM, Sollid S, Kock-Jensen C, Juul N, Eskesen V, Sundstrom T, et al. [Prehospital management of patients with severe head injuries. Scandinavian guidelines according to Brain Trauma Foundation]. Lakartidningen 2008;105:1834-8.
- Socialstyrelsen. Klassifikation av funktionstillstånd, funktionshinder och hälsa. Svensk version av International Classification of Functioning, Disability and Health (ICF). ISBN 91-7201-755. Artikelnr 2003-4-1. 2003.
- Carroll LJ, Cassidy JD, Peloso PM, Borg J, von Holst H, Holm L, et al. Prognosis for mild traumatic brain injury: results of the WHO Collaborating Centre Task Force on Mild Traumatic Brain Injury. J Rehabil Med 2004:84-105.
- Esteban-Cornejo I, Tejero-Gonzalez CM, Sallis JF, Veiga OL. Physical activity and cognition in adolescents: A systematic review. J Sci Med Sport 2015;18:534-9.
- Hotting K, Roder B. Beneficial effects of physical exercise on neuroplasticity and cognition. Neurosci Biobehav Rev 2013;37:2243-57.
- Eapen BC, Allred DB, O'Rourke J, Cifu DX. Rehabilitation of moderate–to–severe traumatic brain injury. Semin Neurol 2015;35:e1-3.
- Horn SD, DeJong G, Smout RJ, Gassaway J, James R, Conroy B. Stroke rehabilitation patients, practice, and outcomes: is earlier and more aggressive therapy better? Arch Phys Med Rehabil 2005;86:S101-S114.
- Strandberg T. Case management–relationsarbete inom rehabilitering av personer med förvärvad hjärnskada. In: Bruhn A, Källström Å, Relationer i socialt arbete: gränslandet mellan profession och person. Stockholm 2018.
- Orsén K. Hjärnskadekoordinator – en länk när samordningen brister. Hjärnkraft, 2016;3:14-17.
- Hillborg H. Case management – ett arbetssätt inom socialpsykiatrin. In: Förhållningssätt och möten – Arbetsmetoder i social omsorg. Lund: Studentlitteratur; 2011. p 239-56.
- Hjärnskadekoordinator i Region Skåne – uppbyggnad, erfarenheter och framtidsperspektiv. [Internet] Tillgänglig från: https://vardgivare.skane.se/siteassets/1.-vardriktlinjer/regionala-vardprogram---fillistning/hjarnskadekoordinatorer-bulletin-forord2019.pdf Nedladdad 191008.
- ACI. Agency for Clinical Innovation. Brain Injury Rehabilitation Directorate – NSW Brain Rehabilitation Program: Case Management Model of Care. ISBN: 978-1-76000-226-8. [Internet] Tillgänglig från: https://www.aci.health.nsw.gov.au/. Nedladdad 2019-10-15.
- Lag om stöd och service till vissa funktionshindrade. (1993:387). [Internet] Tillgänglig från https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-1993387-om-stod-och-service-till-vissa_sfs-1993-387. Nedladdad 20190828.
- Socialtjänstlag (2001:453). [Internet] Tillgänglig från: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/socialtjanstlag-2001453_sfs-2001-453 Nedladdad 2019-10-25.
- Lag (1993:387) om stöd och service till vissa funktionshindrade. Insatser för särskilt stöd och särskild service §9. [Internet] Tillgänglig från https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-1993387-om-stod-och-service-till-vissa_sfs-1993-387. Nedladdad 2019-10-25.
- Socialtjänstlag (2001:453), 4 kap. Rätten till bistånd. 1 §. [Internet] Tillgänglig från: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/socialtjanstlag-2001453_sfs-2001-453. Nedladdad 190807.
- Lag (1993:387) om stöd och service till vissa funktionshindrade. 7 § Rätten till insatser. [Internet] Tillgänglig från: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/lag-1993387-om-stod-och-service-till-vissa_sfs-1993-387 Nedladdad: 190708.
- Bootes K, Chapparo CJ. Cognitive and behavioural assessment of people with traumatic brain injury in the work place: occupational therapists' perceptions. Work 2002;19:255-68.
- Frostad Liaset I, Loras H. Perceived factors in return to work after acquired brain injury: A qualitative meta-synthesis. Scand J Occup Ther 2016;23:446-57.
- Stergiou-Kita M, Yantzi A, Wan J. The personal and workplace factors relevant to work readiness evaluation following acquired brain injury: Occupational therapists’ perceptions. Brain Injury 2010;24:948-58.
- Desouza M, Sycamore M, Little S, Kirker SGB. The Papworth Early Rehabilitation Programme: Vocational outcomes. Disab Rehabil 2007;29:671-77.
- Holmqvist K, Ivarsson A-B, Holmefur M. Occupational therapist practice patterns in relation to clients with cognitive impairment following acquired brain injury. Brain Injury 2014;28:1365-73.
- Ståhl C. Arbetsrehabiliteringens aktörer och roller–ett systemteoretiskt perspektiv. In: Ekberg K, Eklund M, Hensing G, editors. Återgång i arbete: Processer, bedömningar, åtgärder. 1 ed. Lund: Studentlitteratur; 2015. p 233.
- Saunders SL, Nedelec B. What work means to people with work disability: a scoping review. J Occup Rehabil 2014;24:100-10.
- Schipper K, Visser-Meily JMA, Hendrikx A, Abma T. Participation of people with acquired brain injury: Insiders perspectives. Brain injury : [BI] 2011;25:832-43.
- Hall A, Grohn B, Nalder E, Worrall L, Fleming J. A Mixed Methods Study of the Experience of Transition to the Community of Working-Aged People with Non-Traumatic Brain Injury. Brain Impairment 2012;13
- van Velzen JM, van Bennekom CA, Edelaar MJ, Sluiter JK, Frings-Dresen MH. How many people return to work after acquired brain injury?: a systematic review. Brain Inj 2009;23:473-88.
- Jackson M, Harkess J, Ellis J. Reporting Patients’ Work Abilities: How the Use of Standardised Work Assessments Improved Clinical Practice in Fife. British Journal of Occupational Therapy 2004;67
- Vahlne Westerhäll Lea. Rehabiliteringsvetenskap, Rehabilitering till arbetslivet i ett flerdisciplinärt perspektiv. Lund, Studentlitteratur; 2006
- Fadyl JK, McPherson KM. Approaches to vocational rehabilitation after traumatic brain injury: a review of the evidence. J Head Trauma Rehabil 2009;24:195–212.
- Tyerman A. Vocational rehabilitation after traumatic brain injury: models and services. NeuroRehabilitation 2012;31:51-62.
- Ponsford J, Harrington H, Olver J, Roper M. Evaluation of a community-based model of rehabilitation following traumatic brain injury. Neuropsychol Rehabil 2006;16:315-28.
- Powell J, Heslin J, Greenwood R. Community based rehabilitation after severe traumatic brain injury: a randomised controlled trial. J Neurol Neurosurg Psychiatry 2002;72:193-202.
- SBU:s Metodbok Utvärdering av metoder i hälso- och sjukvården och insatser i socialtjänsten. En handbok. [Internet] Tillgänglig från: https://www.sbu.se/contentassets/d12fd955318f4feab3709d7ebcc9a72b/sbushandbok.pdf. Nedladdad: 190709.
- Willman A, Stoltz P, Bahtsevani C. Evidensbaserad omvårdnad : en bro mellan forskning & klinisk verksamhet. Lund, Studentlitteratur; 2011; ISBN 9789144056449.
- Rayyan QCRI. Tillgängligt från: https://rayyan.qcri.org/welcome. Nedladdad 2019-11-25.
- Sterne JA, Hernan MA, Reeves BC, Savovic J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. Bmj 2016;355:i4919.
- Review Manager (RevMan) [Computer program]. Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
- Puhan MA, Frey M, Buchi S, Schunemann HJ. The minimal important difference of the hospital anxiety and depression scale in patients with chronic obstructive pulmonary disease. Health Qual Life Outcomes 2008;6:46.
- Chan KS, Aronson Friedman L, Bienvenu OJ, Dinglas VD, Cuthbertson BH, Porter R, et al. Distribution-based estimates of minimal important difference for hospital anxiety and depression scale and impact of event scale-revised in survivors of acute respiratory failure. General Hospital Psychiatry 2016;42:32-35.
- Cole TB, Flanagin A. Recovery after violence and human rights abuses. JAMA: Journal of the American Medical Association 2013;310:486-87.
- Chen P, Lin KC, Liing RJ, Wu CY, Chen CL, Chang KC. Validity, responsiveness, and minimal clinically important difference of EQ-5D-5L in stroke patients undergoing rehabilitation. Qual Life Res 2016;25:1585-96.
- Cochrane. Cochrane Handbook for Systematic Reviews of Interventions. Tillgänglig från: http://handbook-5-1.cochrane.org/. Nedladdad 190709.
- Finfgeld-Connett D. Use of content analysis to conduct knowledge-building and theory-generating qualitative systematic reviews. Qualitative Research 2013;14:341-52.
- GRADE. The GRADE working group. [Internet] Tillgänglig från: http://www.gradeworkinggroup.org/. Nedladdad 190906.
- Salazar AM, Warden DL, Schwab K, Spector J, Braverman S, Walter J, et al. Cognitive rehabilitation for traumatic brain injury: A randomized trial. Defense and Veterans Head Injury Program (DVHIP) Study Group. Jama 2000;283:3075–81.
- Andelic N, Bautz-Holter E, Ronning P, Olafsen K, Sigurdardottir S, Schanke AK, et al. Does an early onset and continuous chain of rehabilitation improve the long-term functional outcome of patients with severe traumatic brain injury? J Neurotrauma 2012;29:66-74.
- Mackay L, Bernstein B, Chapman P, Morgan A, Milazzo L. Early intervention in severe head injury: long-term benefits of a formalized program. Arch Phys Med Rehabil 1992;73(7):635-41.
- Mohamed WRA, Leach MJ, Reda NA, Abd‐Ellatif MM, Mohammed MA, Abd‐Elaziz MA. The effectiveness of clinical pathway‐directed care on hospitalisation‐related outcomes in patients with severe traumatic brain injury: A quasi‐experimental study. J Clin Nurse 2018;27:e820-32.
- Niemeier JP, Kreutzer JS, Marwitz JH, Gary KW, Ketchum JM. Efficacy of a brief acute neurobehavioural intervention following traumatic brain injury: a preliminary investigation. Brain Inj 2011;25:680-90.
- Semlyen JK, Summers SJ, Barnes MP. Traumatic brain injury: efficacy of multidisciplinary rehabilitation. Arch Phys Med Rehabil 1998;79:678-83.
- Brenner LA, Forster JE, Hoffberg AS, Matarazzo BB, Hostetter TA, Signoracci G, et al. Window to Hope: A Randomized Controlled Trial of a Psychological Intervention for the Treatment of Hopelessness Among Veterans With Moderate to Severe Traumatic Brain Injury. J Head Trauma Rehabil 2018;33:E64-e73.
- Hsieh MY, Ponsford J, Wong D, Schonberger M, Taffe J, McKay A. Motivational interviewing and cognitive behaviour therapy for anxiety following traumatic brain injury: a pilot randomised controlled trial. Neuropsychol Rehabil 2012;22:585-608.
- Goranson TE, Graves RE, Allison D, La Freniere R. Community integration following multidisciplinary rehabilitation for traumatic brain injury. Brain Inj 2003;17:759-74.
- Sarajuuri JM, Kaipio ML, Koskinen SK, Niemela MR, Servo AR, Vilkki JS. Outcome of a comprehensive neurorehabilitation program for patients with traumatic brain injury. Arch Phys Med Rehabil 2005;86:2296-302.
- Svendsen HA, Teasdale TW. The influence of neuropsychological rehabilitation on symptomatology and quality of life following brain injury: a controlled long-term follow-up. Brain Inj 2006;20:1295-306.
- Bell KR, Fann JR, Brockway JA, Cole WR, Bush NE, Dikmen S, et al. Telephone Problem Solving for Service Members with Mild Traumatic Brain Injury: A Randomized, Clinical Trial. J Neurotrauma 2017;34:313-21.
- Bryant RA, Moulds M, Guthrie R, Nixon RD. Treating acute stress disorder following mild traumatic brain injury. Am J Psychiatry 2003;160:585-7.
- Potter SD, Brown RG, Fleminger S. Randomised, waiting list controlled trial of cognitive-behavioural therapy for persistent postconcussional symptoms after predominantly mild-moderate traumatic brain injury. J Neurol Neurosurg Psychiatry 2016;87:1075-83.
- Richardson JS, Fann JR, Bell KR, Temkin N. Impact of Telephone-Based Problem-Solving Treatment on the Use of Medical and Psychological Services in the Military. J Head Trauma Rehabil 2017;33:2:E1-E6.
- Rytter HM, Westenbaek K, Henriksen H, Christiansen P, Humle F. Specialized interdisciplinary rehabilitation reduces persistent post-concussive symptoms: a randomized clinical trial. Brain Inj 2019;33:266-81.
- Scheenen ME, Visser-Keizer AC, de Koning ME, van der Horn HJ, van de Sande P, van Kessel M, et al. Cognitive Behavioral Intervention Compared to Telephone Counseling Early after Mild Traumatic Brain Injury: A Randomized Trial. J Neurotrauma 2017;34:2713-20.
- Silverberg ND, Hallam BJ, Rose A, Underwood H, Whitfield K, Thornton AE, et al. Cognitive-behavioral prevention of postconcussion syndrome in at-risk patients: a pilot randomized controlled trial. J Head Trauma Rehabil 2013;28:313-22.
- Tiersky LA, Anselmi V, Johnston MV, Kurtyka J, Roosen E, Schwartz T, et al. A trial of neuropsychologic rehabilitation in mild-spectrum traumatic brain injury. Arch Phys Med Rehabil 2005;86:1565-74.
- Twamley EW, Thomas KR, Gregory AM, Jak AJ, Bondi MW, Delis DC, et al. CogSMART Compensatory Cognitive Training for Traumatic Brain Injury: Effects Over 1 Year. J Head Trauma Rehabil 2015;30:391-401.
- Vikane E, Hellstrom T, Roe C, Bautz-Holter E, Assmus J, Skouen JS. Multidisciplinary outpatient treatment in patients with mild traumatic brain injury: A randomised controlled intervention study. Brain Inj 2017;31:475-84.
- Hanks RA, Rapport LJ, Wertheimer J, Koviak C. Randomized controlled trial of peer mentoring for individuals with traumatic brain injury and their significant others. Arch Phys Med Rehabil 2012;93:1297-304.
- Trexler LE, Parrott DR, Malec JF. Replication of a Prospective Randomized Controlled Trial of Resource Facilitation to Improve Return to Work and School After Brain Injury. Arch Phys Med Rehabil 2016;97:204-10.
- Greenwood RJ, McMillan TM, Brooks DN, Dunn G, Brock D, Dinsdale S, et al. Effects of case management after severe head injury. Bmj 1994;308:1199-205.
- Hopman K, Tate RL, McCluskey A. Community-based rehabilitation following brain injury: Comparison of a transitional living program and a home-based program. Brain Impairment 2012;13:44-61.
- Willer B, Button J, Rempel R. Residential and home-based postacute rehabilitation of individuals with traumatic brain injury: a case control study. Arch Phys Med Rehabil 1999;80:399-406.
- Sloan S, Callaway L, Winkler D, McKinley K, Ziino C. Accommodation outcomes and transitions following community-based intervention for individuals with acquired brain injury. Brain Impairment 2012;13:24-43.
- Doig E, Fleming J, Kuipers P, Cornwell P, Khan A. Goal-directed outpatient rehabilitation following TBI: a pilot study of programme effectiveness and comparison of outcomes in home and day hospital settings. Brain Inj 2011;25:1114-25.
- Man DW, Poon WS, Lam C. The effectiveness of artificial intelligent 3-D virtual reality vocational problem-solving training in enhancing employment opportunities for people with traumatic brain injury. Brain Inj 2013;27:1016-25.
- Ownsworth T, Fleming J, Shum D, Kuipers P, Strong J. Comparison of individual, group and combined intervention formats in a randomized controlled trial for facilitating goal attainment and improving psychosocial function following acquired brain injury. J Rehabil Med 2008;40:81-8.
- Radford K, Sutton C, Sach T, Holmes J, Watkins C, Forshaw D, et al. Early, specialist vocational rehabilitation to facilitate return to work after traumatic brain injury: the FRESH feasibility RCT. Health Technol Assess 2018;22:1-124.
- Radford K, Phillips J, Drummond A, Sach T, Walker M, Tyerman A, et al. Return to work after traumatic brain injury: cohort comparison and economic evaluation. Brain Inj 2013;27:507-20.
- CCEMG EPPI-Centre Cost Converter v.1.6 [Internet] Tillgänglig från: https://eppi.ioe.ac.uk/costconversion/. Nedladdad 2019-09-07.
- Richardson JS, Guzauskas GF, Fann JR, Temkin NR, Bush NE, Bell KR, et al. Economic evaluation of telephone-based concussion management for combat-related mild traumatic brain injury. J Telemed Telecare 2018;24:282-89.
- van Heugten CM, Geurtsen GJ, Derksen RE, Martina JD, Geurts ACH, Evers SMAA. Intervention and societal costs of residential community reintegration for patients with acquired brain injury: a cost-analysis of the brain integration programme. J Rehabil Med 2011;43:647-52.
- Geurtsen GJ, Martina JD, Van Heugten CM, Geurts AC. A prospective study to evaluate a new residential community reintegration programme for severe chronic brain injury: the Brain Integration Programme. Brain Inj 2008;22:545-54.
- Copley A, McAllister L, Wilson L. We finally learnt to demand: Consumers’ access to rehabilitation following traumatic brain injury. Brain Impairment 2013;14:436-49.
- D'Cruz K, Unsworth C, Roberts K, Morarty J, Turner-Stokes L, Wellington-Boyd A, et al. Engaging patients with moderate to severe acquired brain injury in goal setting. International Journal of Therapy & Rehabilitation 2016;23:20-31.
- O'Callaghan A, McAllister L, Wilson L. Insight vs readiness: Factors affecting engagement in therapy from the perspectives of adults with TBI and their significant others. Brain Injury 2012;26:1599-1610.
- Turner B, Fleming J, Cornwell P, Worrall L, Ownsworth T, Haines T, et al. A qualitative study of the transition from hospital to home for individuals with acquired brain injury and their family caregivers. Brain Inj 2007;21:1119-30.
- Turner BJ, Fleming J, Ownsworth T, Cornwell P. Perceived service and support needs during transition from hospital to home following acquired brain injury. Disability and rehabilitation 2011;33(10):818-29.
- Abrahamson V, Jensen J, Springett K, Sakel M. Experiences of patients with traumatic brain injury and their carers during transition from in-patient rehabilitation to the community: a qualitative study. Disabil Rehabil 2017;39:1683-94.
- Mueller C, Wang Y, Brooks A, Morant N, Sullivan P, Raymont V. 'Attending to the wound and the person' - patients' experiences and expectations of a newly established traumatic brain injury clinic. Brain Inj 2017;31:1863-70.
- Graff HJ, Christensen U, Poulsen I, Egerod I. Patient perspectives on navigating the field of traumatic brain injury rehabilitation: a qualitative thematic analysis. Disabil Rehabil 2018;40:926-34.
- Lexell EM, Alkhed A-K, Olsson K. The group rehabilitation helped me adjust to a new life: Experiences shared by persons with an acquired brain injury. Brain Injury 2013;27:529-37.
- Lewin S, Glenton C, Munthe-Kaas H, Carlsen B, Colvin CJ, Gulmezoglu M, et al. Using qualitative evidence in decision making for health and social interventions: an approach to assess confidence in findings from qualitative evidence syntheses (GRADE-CERQual). PLoS Med 2015;12:e1001895.
- Munthe-Kaas H, Bohren MA, Glenton C, Lewin S, Noyes J, Tuncalp O, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 3: how to assess methodological limitations. Implement Sci 2018;13:9.
- Colvin CJ, Garside R, Wainwright M, Munthe-Kaas H, Glenton C, Bohren MA, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings-paper 4: how to assess coherence. Implement Sci 2018;13:13.
- Noyes J, Booth A, Lewin S, Carlsen B, Glenton C, Colvin CJ, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings–paper 6: how to assess relevance of the data. Implement Sci 2018;13:4.
- Glenton C, Carlsen B, Lewin S, Munthe-Kaas H, Colvin CJ, Tunçalp Ö, et al. Applying GRADE-CERQual to qualitative evidence synthesis findings—paper 5: how to assess adequacy of data. Implement Sci 2018;13:14.
- Hälso- och sjukvårdslagen (2017:30), 2 §. [Internet] Tillgänglig från: https://www.riksdagen.se/sv/dokument-lagar/dokument/svensk-forfattningssamling/halso--och-sjukvardslag_sfs-2017-30. Nedladdad 20190828.
- Hjärnkraft. Kartläggning av hjärnskaderehabilitering. [Internet] Tillgänglig från: http://www.hjarnkraft.nu/sv/vart_arbete/kartlaggning_av_hjarnskaderehabilitering Nedladdad: 190709.
- Hultcrantz M, Rind D, Akl EA, Treweek S, Mustafa RA, Iorio A, et al. The GRADE Working Group clarifies the construct of certainty of evidence. J Clin Epidemiol 2017.
- van Tulder M, Furlan A, Bombardier C, Bouter L. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine (Phila Pa 1976) 2003;28:1290-9.
- IVO. Inspektionen för vård och omsorg. Vad har IVO sett 2018? Iakttagelser och slutsatser om vårdens och omsorgens brister för verksamhetsåret 2018. [Internet] Tillgänglig från: https://www.ivo.se/globalassets/dokument/publicerat/rapporter/rapporter-2019/vad-har-ivo-sett-2018-digital.pdf. Nedladdad 2019-09-07. 2019.
- Vårdanalys. Från mottagare till medskapare. Ett kunskapsunderlag för en mer personcentrerad hälso- och sjukvård. Rapport 2018:8. ISBN 978-91-87213-90-8.
- Plant SE, Tyson SF, Kirk S, Parsons J. What are the barriers and facilitators to goal-setting during rehabilitation for stroke and other acquired brain injuries? A systematic review and meta-synthesis. Clin Rehabil 2016;30:921-30.
- Hjärnkraft. Modellprojektet. För livslång, individanpassad rehabilitering, stöd & service. Hjärnskadeförbundet Hjärnkraft. [Internet] Tillgänglig från: http://www.levamedtraumatiskhjarnskada.se/. Nedladdad 2019-09-07.
- Richardson J, Iezzi A, Maxwell A. Sharing and the Provision of "Cost-Ineffective" Life-Extending Services to Less Severely Ill Patients. Value Health 2018;21:951-957.