Interventions to prevent misuse of alcohol, drugs and gambling in youth
 Share on Facebook
Share on Facebook
 Share on LinkedIn
Share on LinkedIn
 Share via Email
Share via Email
Background
Use of alcohol, illicit drugs, doping substances, tobacco and gambling (ANDTG) are common among young people. A large number of interventions have been developed for prevention, but the evidence for them is unclear.
Objectives
The aim of this systematic review was to assess the effects of interventions to prevent misuse of alcohol, tobacco, illicit drugs and gambling in youth below 25 years. Interventions that aimed to change behavior (programs, mass media campaigns) or access (price, legislation, policies) were assessed. Both positive and negative (iatrogenic) effects were considered. This review also included health economic aspects, including a model analysis of the potential cost-effectiveness of preventing alcohol binge drinking.
Method
The systematic review was conducted in accordance with the methodology developed by the Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU). Systematic reviews, randomized and nonrandomized controlled studies (RCT, NRCT) or interrupted time series studies (ITS) in English or Scandinavian languages and published 1990 or later were eligible for inclusion. Outcomes of interest were onset of use, consumption, drug related harm or binge drinking, measured at least six months after end of intervention. Only studies with low to moderate risk for bias were included in the analyses. The certainty of the evidence for the effects was assessed with GRADE.
Results
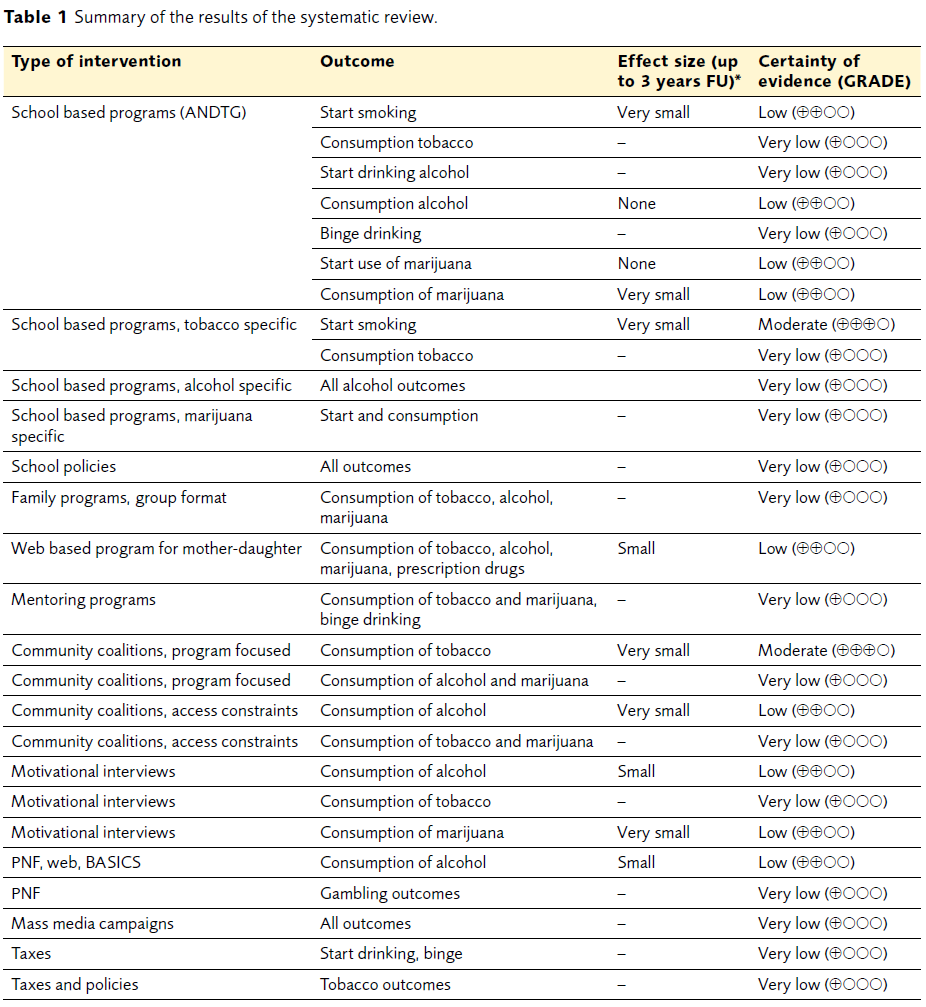
The results, categorized after type of intervention, are summarized in Table 1. A major finding was that school based programs claiming to be generally drug preventive could at best prevent the misuse of a single drug. Another major finding was that no type of intervention could prevent alcohol or marijuana-use onset. Intervention effects were mostly very small or small, with effect sizes (RD or Cohen’s d) in the 1–5% range. Furthermore, most studies evaluating legislative actions, e.g. taxes, had a high risk for bias and no conclusions could be drawn.
Health economic analysis
The literature reviews on cost-effectiveness analyses of specific school based programs and of information campaigns concluded that no analyses relevant for contemporary Swedish settings are available.
A health economic model was constructed to enable cost-effectiveness analyses of alcohol prevention measures. The Markov model simulates the alcohol consumption patterns of young people aged 11 to 24 years, using the health states No Consumption, Consumption, Binge Drinking, and Death. Swedish epidemiological data was used to estimate the annual age-specific probabilities for young people to move to the Consumption state and to engage in Binge Drinking. The consequences of Binge Drinking included alcohol poisoning, accidents and violence, including related societal costs. Health effects were expressed as QALYs. An assumed 0.05 loss of quality-of-life from Binge Drinking was deducted from the assumed quality-of-life of 1 in the No Consumption and Consumption health states. Costs and QALYs were discounted 3%.
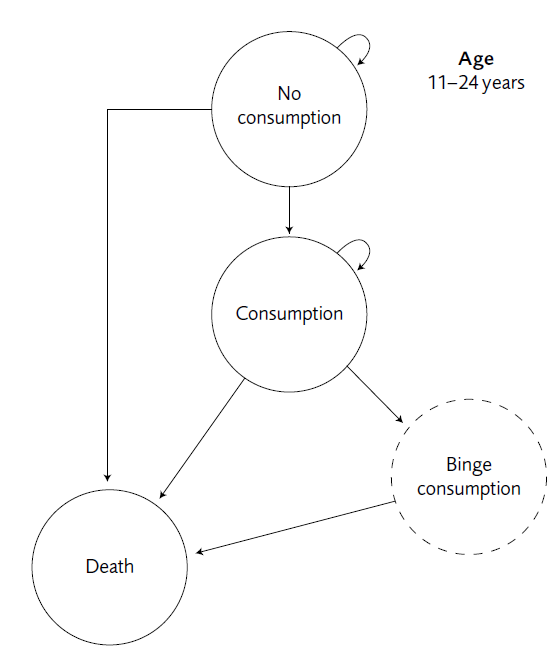
Figure 1. Health states in the Markov model.
This alcohol model was used for a threshold analysis, based on a cost-effectiveness willingness-to-pay threshold of 500 000 SEK per QALY. Two effective interventions, one specific school based program and MI (motivational interviewing), were assumed to decrease binge drinking for one year after the intervention.
The school based program, delivered at age 13 years, needed to reduce binge drinking among 14-year olds with at least 5% (i.e from a prevalence of 40% binge drinking among those that consume alcohol to a prevalence of 38%) to become cost-effective. The MI, given in a primary care setting to youths aged 18 years with a problem drinking behavior, needed to reduce binge drinking by 2.5% (from a prevalence of 60% of consumers to 58.5%).
Consequences
Although there are a vast number of studies evaluating prevention interventions, few interventions have been able to demonstrate that they can deter young people from using ANDTG, and effect sizes are small or very small. Thus there is a need for new interventions, possibly based on other behavioral theories or delivered in other arenas.
Conclusions
- None of the structured school based programs can prevent drug use in general. A few programs can reduce the consumption of tobacco or cannabis, or reduce binge drinking. The effects are usually between 1 and 5%. There was insufficient evidence to draw any conclusions on programs using structured family support groups. Some studies reported increased consumption after school or parental support programs.
- When implemented correctly, broadly coordinated community coalitions that limit young people’s access to alcohol in multiple ways (i.e. licensing, restricting opening hours), may reduce their alcohol consumption. However, multimodal community programs aimed at changing attitudes, norms or behaviors, have little or no effect on the amount of alcohol, cannabis or tobacco young people consume.
- Brief interventions such as motivational interviews (MI) or personalized normative feedback may reduce alcohol consumption by young people who engage in hazardous drinking.
- The model based health economic analysis of alcohol prevention estimates that two preventive interventions may cost less than 500 000 SEK per QALY. A structured school based program may be cost effective, provided that the proportion of binge drinking youth is reduced by at least 5%. MI may be cost effective provided that the proportion of binge drinking youth is reduced by at least 2.5%.
- Despite the vast number of studies evaluating interventions to prevent or reduce drug and alcohol abuse, there continues to be significant knowledge gaps. There is a need for interventions other than the structured programs evaluated to be developed and assessed in well-designed studies. Further research is also needed that focuses on young adults in non-school settings, as well as research focused on the hazardous use of performance enhancing drugs, prescription medications and gambling.
How to cite this report: SBU. Interventions to prevent misuse of alcohol, drugs and gambling in youth. Stockholm: Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU); 2015. SBU report no 243 (in Swedish).
Project group
Experts
- Kent Nilsson (Chair, Professor, Västerås)
- Johanna Gripenberg (PhD, Stockholm)
- Johan Jarl (PhD, Lund)
- Gunilla Jarlbro (Professor, Lund)
- Christina Kadesjö (PhD, Gothenburg)
- Ingvar Karlberg (Professor, Gothenburg)
- Josef Milerad (Assiociate Professor, Stockholm)
- Fredrik Spak (Assiociate Professor, Gothenburg)
- Nils Stenström (PhD, Stockholm)
- Anders Tengström (PhD, Stockholm)
SBU
- Agneta Pettersson (Projekt Manager)
- Agneta Brolund (Information Specialist)
- Kickan Håkanson (Project Administrator)
- Pia Johansson (Health Economist)
- Jenny Odeberg (Assisting Project Manager)