Early diagnosis of symptomatic cancer
 Share on Facebook
Share on Facebook
 Share on LinkedIn
Share on LinkedIn
 Share via Email
Share via Email
Background
Early diagnosis of cancer is one of the main objectives of the current Swedish cancer strategy. The government has thus commissioned the Swedish Council on Technology Assessment in Health Care (SBU) to in a systematic review evaluate if there are any scientifically proven methods, excluding screening, that can be used for the early and accurate diagnosis of cancer.
Objective
The objective of this systematic review was to assess the scientific basis for methods that might provide earlier cancer diagnosis in persons with symptoms or signs that might indicate cancer. Screening for cancer was not included in this assessment.
Delay in treatment is often defined as the patient, doctor, or system delay according to the phase in which the delay occurs. Patient delay is usually understood to be the time from the first symptoms to the first contact with the health care system. Such delay usually occurs due to neglect, fear of a serious disease, or not wanting to bother the doctor. Doctor delay is used to describe the delay that occurs due to mistakes, poor understanding of the patient’s symptoms, negligence, etc. System delay occurs due to poor organisation of the health care system or a lack of resources. These delays are usually assumed to occur in sequence one after another. Our understanding, however, is that the different delays overlap and sometimes can be difficult to separate from each other (figure 1). System delay can occur in all phases depending on how the management is organised, how resources are allocated and utilised, etc. For instance, poor accessibility to primary care caused by poor organisation or lack of resources can result in a person with symptoms choosing not to seek care at all. In this report, we focus on interventions that might shorten the time from the first symptom to the diagnosis in ambulatory care. Delays can, of course, also occur later in the course of the patient’s management, but such delays are not discussed in this report.
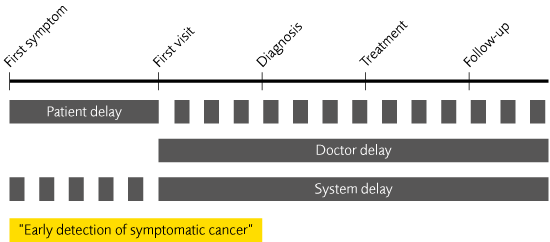
Figure 1. The components of delay.
Method
A systematic review was undertaken following the standard methods used by the SBU. The review focused on patient’, doctor, and system delay from the first experience of symptoms and signs to the diagnosis of cancer in ambulatory care. We investigated interventions such as education, information, fast-tracks, guidelines, IT systems, structured referrals, telemedicine, etc. Outcomes were different lengths of time for the diagnostic process, the stage distribution at diagnosis, and survival rates. The evaluation included medical, economic, social, and ethical aspects of the different interventions.
Conclusions
- Adding a photograph of suspected skin cancer to the standard referral can shorten the time to the initial evaluation by a specialist department. The management of the patient can also be better planned and resources can be saved.
- Providing information and education to the population can improve knowledge and awareness of cancer, especially if the intervention is personalised and this can be seen up to 2 years after the intervention. Studies with longer follow-up times are lacking.
- We could not determine if providing information and education to health care professionals led to that patients are diagnosed earlier cancer diagnosis or that such interventions had any impact on survival or mortality. The scientific basis was insufficient in this respect.
- Fast-tracks for managing persons with certain defined symptoms that are indicative of cancer can shorten the diagnostic phase by a number of weeks. However, most new cases are discovered as part of routine patient care outside the fast-tracks. There are some indications that the diagnostic time of those in routine care is actually increased when fast-tracks are introduced into the health care system. The risk for such delay for patients in routine care must be addressed when fast-tracks are introduced and evaluated.
- Self-examinations of breasts do not affect breast cancer mortality on a population level but do increase the rate of local diagnostic procedures.
- Cost-effectiveness could not be evaluated for any of the methods because of a lack of information in the literature.
Knowledge gaps
- The prevalence of symptoms indicative of a possible cancer in the Swedish population are not known nor is it known how many persons are investigated for possible cancer in Sweden.
- The effects on management and prognostic factors by providing information and education to professionals in the health care system need to be better studied.
- Better studies are needed to evaluate the effects of different fast-track strategies.
Ethical and social aspects
In general, we need better knowledge on the psychological and social effects of different methods aiming to speed up cancer diagnosis. Intense information and education of the population as well as the introduction of fast-tracks might lead to reallocation or competition for resources that might actually increase delays for those who are not part of these interventions. This must be avoided.
How to cite this report: SBU. Early diagnosis of symptomatic cancer. Stockholm: Swedish Council on Health Technology Assessment (SBU); 2014. SBU report no 222 (in Swedish).